Checking the health and maximum capacity of the battery in your beloved iPad isn’t as easy as it should be, but we can walk you through the process.
Finding out how worn out the tablet’s battery is can help you decide if it’s time for a new model.
Explaining iPad battery health: maximum capacity vs. cycles
Diamonds are forever but batteries are not. Li-ion batteries in phones, laptops, etc., inevitably wear out. Each one comes with a limited number of times it can be charged and discharged, which is called a cycle. But every time you plug in the device isn’t the start of a new cycle. One starts only after all of the battery’s power has been expended.
“You could use half of your laptop’s charge in one day, and then recharge it fully,” explains Apple. “If you did the same thing the next day, it would count as one charge cycle, not two. In this example, it might take several days to complete a cycle.”
This is where a measurement of maximum capacity comes in. This indicates how much power your iPad battery can hold now compared to the capacity when it was new. It’s typically listed as a percentage, and is a much better indication of battery health.
Here’s how to find out what the maximum capacity is for your iPad’s battery.
How to check battery health and maximum capacity on your iPad
On an iPhone, you can discover the maximum battery capacity with a quick visit to the Battery area in Settings. iPadOS doesn’t make it nearly so easy. The information is in there — you just need to dig it out.
Open the Privacy & Security then Analytics & Improvements sections of Settings to get access to iPad battery health data. Screenshot: Ed Hardy/Cult of Mac
Start by going to Settings -> Privacy & Security -> Analytics & Improvements. On that screen, make sure Share iPad Analytics is toggled on.
Then tap on Analytics Data. This will open a long list of files keeping track of the minutia of your iPad. You’re looking for one whose name starts with “Analytics-” followed by today’s date (or the most recent one available). Tap on it to open the file. You’ll see a long, long series of entries, 99.999% of which is useless to you. But the data you want is buried in there.
Note: if you’re using an older version of iPadOS, you might be looking for a file that starts with “log-aggregated-” or maybe “sysdiagnose_” instead.
From here, there are two ways to go: use a Shortcut to find the current maximum capacity of your iPad’s battery or search through the file on your own.
1. Try a Shortcut
Install and open the Battery Stats Shortcut to discover your iPad’s battery health. Screenshot: Ed Hardy/Cult of Mac
If you’re willing to install a Shortcut on your iPad, follow this link to Battery Stats then click Add Shortcut. (I went through the code and it doesn’t do anything dodgy.)
Now go back and open that specific analytics file you found earlier in Settings. Tap on the Share Menu icon (box with an arrow point up) in the upper righthand corner of the screen, then select Battery Stats from the resulting popup window.
After a few seconds, a window will open showing you the battery capacity in both mAh and a percentage.
2. Search for yourself
Try to find these codewords in the iPad analytics file. Screenshot: Ed Hardy/Cult of Mac
Alternatively, you can search through the lengthy analytics file for the data on your own. You’re looking for “MaximumCapacityPercent” and “CycleCount.”
It’s not hard to guess that the first number is Apple’s estimate of the maximum current capacity of your iPad battery. Though you can calculate this for yourself. Go back to the analytics file and look for NominalChargeCapacity and MaximumFCC, then calculate:
(MaximumFCC / NominalChargeCapacity) * 100
This is generally lower than MaximumCapacityPercent. Oddly, that figure is often over 100% if the iPad is new. I don’t know why.
You’ll have noticed that the analytics file is enormous — you’d be better off opening it in a text editor and using a Find function to search for those terms. I use GoodReader, but there are other options.
To transfer the file to the app of your choice: open the file, tap on the Share Menu icon (box with an arrow point up) in the upper righthand corner of the screen, then select the text editor you prefer from the Share Sheet.
What now?
What happens next depends on your iPad battery’s health as determined by its current maximum capacity percentage. As noted earlier, Apple considers anything over 80% to be healthy.
Above than number, you’re almost certainly good. My iPad is at 88% (or 92%, depending) and I’ve used it virtually every day for about 18 months, so it’s in great shape.
The possible exception is if your tablet is fairly new and the max capacity isn’t near 100%. Before you get concerned, though, check your Cycle Count. If it’s also high (mine is at 165), it means you’re a very heavy user and are putting a lot wear on the battery. That’s not a bad thing — you clearly like the product a lot.
But if your iPad has seen many years of use and its battery health isn’t good — its maximum capacity is at or below 80% — it means the device doesn’t last as long between charges as it used to.
One option is replacing the battery. Apple will do it for roughly $100 to $120 depending on your model, and the process will return the computer to its original battery life.
Or you might look into one of the new iPad Air or iPad Pro models expected soon. (You’ve been looking for a reason to upgrade, right?)
In late 2020, COVID-19’s global death toll was rising as cold weather in the Northern Hemisphere and holiday gatherings spurred rapid transmission of SARS-CoV-2 in the absence of a vaccine. Scientists and public-health officials were desperate for new ways to track the virus, which often moved faster than contact tracers could follow it.
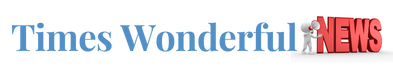
Tong Zhang, an environmental engineer and microbiologist at the University of Hong Kong (HKU), and his colleagues were pioneers of what was fast becoming a popular surveillance method. They had been collecting periodic wastewater samples from about two dozen maintenance holes in the city and testing the sewage for coronavirus DNA, with support from Hong Kong’s government. In late December, they traced an outbreak to a single apartment building where there had been no sign of cases1.
The government quickly took action. Officials tested all of the building’s 2,000-odd residents; 9 tested positive. “Those people were isolated and went to a quarantine site. So they stopped the transmission chain,” Zhang says. After that success, he and his colleagues expanded their efforts.
These scientists traced a new coronavirus lineage to one office — through sewage
Wastewater testing remains part of Hong Kong’s COVID-19 strategy to this day. Zhang’s team tests for the coronavirus at about 20 sites across the city each week, he says, and the team has expanded the analysis of these samples to cover other pathogens, including influenza, rotavirus, norovirus and mpox, as well as markers of antimicrobial resistance. He views wastewater testing as a way to gauge the health of an entire community at once. “If we can make the methodology more standardized”, this tool becomes a “promising and exciting” way to screen the world for pathogens, including those that scientists haven’t yet identified,he says.
Many researchers are following similar approaches. There are currently more than 4,600 sites around the world where wastewater is being collected for SARS-CoV-2 testing, and some of the research teams involved are investigating other potential applications, such as tracking illicit drug use and even the prevalence of cancer.
But whether this has the potential to be an effective public-health strategy is still a matter of debate. Leo Poon, a colleague of Zhang’s at HKU’s School of Public Health, says that more research should be done before health agencies expand their sewage testing programmes and make this surveillance part of their routine budgets. “There’s still a lot unknown,” he says, particularly in terms of testing for pathogens besides SARS-CoV-2. “I think there’s a steep learning curve at the moment: when we detect something, what does it mean?”
By the end of 2020, several studies had shown that levels of coronavirus in public water systems could correlate with the number of COVID-19 cases in the community. For example, researchers at Stanford University in California found that viral levels in wastewater rose and fell with cases in the San Francisco Bay area3. The group that led the work has gone on to found the WastewaterSCAN project, which tests samples from nearly 200 sites across the United States (see ‘Peak transmission’).
Source: WastewaterSCAN
In the most successful wastewater projects, scientists say, researchers collaborated directly with public-health officials, who used the data to inform COVID-19 safety policies. This happened in rural parts of Ghana, where, as in Hong Kong, wastewater testing found COVID-19 cases that hadn’t been caught by other types of surveillance. Habib Yakubu, a public-health researcher at Emory University’s Center for Global Safe Water, Sanitation, and Hygiene in Atlanta, Georgia, worked with a team of Ghanaian scientists to develop testing methods that accounted for the country’s limited public sewers and laboratory equipment. They tried this in two rural districts, Nanumba North and Mion, where government officials suspected that COVID-19 might be spreading but where clinical testing hadn’t identified any cases.
The researchers worked with community leaders to identify sites for sampling, including schools, health-care facilities, markets and streams used for washing clothes. “We looked at, where do people converge?” Yakubu says. COVID-19 was, in fact, present in these regions, the researchers found. As a result, officials increased public-health activities, including community education and vaccination efforts. The team tested for other diseases that are common in Ghana, including cholera and typhoid, which has also informed health actions.
For scientists at the Tata Institute for Genetics and Society in Bengaluru, India, the need for wastewater testing for COVID-19 became clear after the country’s devastating wave of the Delta variant of SARS-CoV-2 in early 2021, says Farah Ishtiaq, an evolutionary ecologist at Tata who leads the COVID-19 surveillance programme in the city. She and her colleagues worked with officials to set up testing at 28 water treatment plants in Bengaluru — a logistically challenging task, because the team had to collect samples manually rather than using the automated samplers common in higher-income nations.
This testing proved its worth during the spread of the Omicron variant in Bengaluru the following year, Ishtiaq says. Wastewater data demonstrated that Omicron variants were spreading widely across the city at a time when data from the health-care system were limited. Officials responded by renewing mask mandates and placing restrictions on large gatherings, she says.
Inspired by case studies such as these, the field has grown drastically over the past 4 years, with hundreds of research teams now testing in 72 countries, according to the COVIDPoops19 dashboard maintained by environmental engineer Colleen Naughton and her colleagues at the University of California, Merced (see ‘Uneven coverage’).
In December 2023 and January 2024, it was clear that COVID-19 was spreading widely in several parts of the world. But public-health agencies had severely cut back on conventional testing and surveillance programmes, leading to uncertainty about how much the coronavirus was spreading, and a sudden focus on wastewater-based epidemiology.
Some scientists and social-media commentators stated that SARS-CoV-2 levels in wastewater correlated with specific case numbers, estimating huge surges in the United States and Europe. But others cautioned that wastewater surveillance is not reliable enough to predict true infection numbers. There’s a “false sense of precision” in such estimates, says Sam Scarpino, an epidemiologist at Northeastern University in Boston, Massachusetts, who has worked on COVID-19 data systems.
Estimates are difficult to make because the sewage data differ considerably from conventional health indicators. In typical surveillance, data represent individual infected people who can be identified through contact tracing, isolated and treated. In wastewater surveillance operations, data can represent entire communities.
COVID variants found in sewage weeks before showing up in tests
They make “a litre represent a million people”, says Douglas Manuel, a public-health physician at the University of Ottawa in Canada. Manuel and his colleagues have identified several variables that can alter results from such screenings; these include population density, precipitation, sample composition, handling and testing methods and quality-control measures4. For example, as snow melts in Ottawa’s spring, it flows into the wastewater system and “scours out” solid waste that might have built up in the pipes, Manuel says. This could interfere with findings relating to SARS-CoV-2 measurements.
To account for those variables, researchers tend to compare measurements from one site over time. The US Centers for Disease Control and Prevention (CDC), for instance, developed a metric called the wastewater viral activity level that compares a testing site’s recent SARS-CoV-2 measurement to past ones, then averages those comparison values across larger regions.
These comparison metrics can be helpful for presenting wastewater results to the public, but they gloss over the data’s complexity. Bilge Kocamemi, an environmental engineer at Marmara University in Istanbul and a project coordinator for Turkey’s wastewater testing, says that she quickly realized that “scientific representation of the data makes the data unusable for the public”. Instead, she and her colleagues developed a relatively simple COVID-19 map: testing sites are displayed in different shades of yellow and green, depending on how high SARS-CoV-2 levels are. This coloured scale is not precise, Kocamemi says, but it’s easy for people who don’t have a scientific background to understand.
Improving estimates
Modelling case counts — or other metrics of COVID-19 spread in a community, such as how many people will be hospitalized — from viral levels in wastewater is difficult, but not impossible, say scientists who work on this challenge. Such models would make it easier for health officials to make policy decisions on the basis of sewage data.
The myriad ways sewage surveillance is helping fight COVID around the world
The CDC’s Center for Forecasting and Outbreak Analytics in Washington DC, which launched in 2022, is one group taking on this challenge. Wastewater data are “a really good leading indicator” for COVID-19’s burden on hospitals, says Dylan George, the centre’s director. In February, George and his colleagues released new hospital forecasting models informed by wastewater data, among other metrics (see go.nature.com/43xumbz). Studies have shown that such models are more accurate when they use wastewater data in tandem with data from the health-care system, rather than just one of those sources5.
George cautions that ongoing research will be needed to better understand the connection between virus levels in wastewater and disease levels in a community. For example, some scientists think that virus levels might change as SARS-CoV-2 continues to mutate; a variant known as JN.1 might cause people to shed more virus particles, or shed them for longer compared with previous variants, George says. “I think that’s going to be an active area of research going forward.”
Modellers would like to have more detailed clinical testing data to allow them to make better comparisons between wastewater results and community infections. The challenge is often even greater for researchers testing wastewater for other viruses, says Casandra Philipson, a scientist at Ginkgo Bioworks, a company in Boston that analyses sewage from aeroplanes and airports, along with conducting research into new biosecurity tools. Philipson says that there are decent clinical data available for COVID-19, flu and respiratory syncytial virus. But, she adds, “When you get outside of those three pathogens, there really is a massive data scarcity issue.”
What else can be tested in sewage?
Some scientists are interested in a range of other diseases and health indicators that show up in people’s waste.
Manual wastewater sampling in India.Credit: Environmental Images/Universal Images Group/Shutterstock
Bernd Manfred Gawlik, who coordinates wastewater work at the European Commission’s Joint Research Centre in Brussels, calls wastewater the “dirty blood of the city”, and compares sewage sampling to blood testing. “We are now only starting to understand” how to diagnose this “blood” at the collective level, he says.
One common target of testing is antimicrobial resistance (AMR), an area of wastewater research that pre-dates the pandemic. Ishtiaq, in Bengaluru, says that “AMR is a huge problem in this part of the world”, because many people use unregulated antibiotics. Her research has expanded from COVID-19 testing to a multifaceted, genomic platform that can look for both viral and bacterial infections. Wastewater data will help researchers to understand which pathogens are driving infections and communicate that information to physicians, she says.
Fatma Guerfali, a molecular biologist and bioinformatician at the Pasteur Institute in Tunis, is also tracking AMR in Tunisia, one of the countries considered most at risk. Guerfali says that she and her colleagues are working with the country’s health agency, as well as with research collaborators in other African countries, to determine how best to expand the programme, which started with COVID-19 testing.
How sewage could reveal true scale of coronavirus outbreak
Beyond global targets such as AMR and flu, wastewater testing priorities differ according to local health challenges. Because this testing can pick up a wide variety of pathogens, scientists often consult with health agencies to determine which targets to prioritize. In Louisville, Kentucky, for example, Ted Smith, director of the Center for Healthy Air, Water and Soil at the University of Louisville, and his colleagues are testing for a ‘panvirome panel’ that includes about 30 pathogens of interest to the local health agency. Last year, the testing picked up measles during an outbreak in the state, and health officials used the data to inform vaccination programmes, alerts for physicians and other health efforts, he says.
Another area of expansion lies in testing chemicals that people excrete into wastewater. Some researchers, such as those at the start-up company Biobot Analytics in Cambridge, Massachusetts, are screening for opioids and other drugs with a risk of misuse. Smith and his colleagues are testing sewage for compounds indicative of exposure to air pollution and they have started research into lead levels. “Every day, we come up with new things that we can interrogate wastewater for,” he says.
A few researchers are even going beyond diseases spread by humans to those spread by animals. In 2022, scientists published work linking new SARS-CoV-2 variants in New York City’s wastewater to the city’s rats6. Ishtiaq is looking at avian flu in Bengaluru, and Ekta Patel, a scientist at the International Livestock Research Institute in Kenya, is studying animal diseases there.
Patel and her colleagues are sampling sewage at slaughterhouses and testing for 66 pathogens, including anthrax, brucellosis, and Rift Valley fever. To complement the wastewater tests, Patel hopes her team can collect data from veterinary clinics and community hospitals.
Some wastewater scientists reflect on how different the early days of the COVID-19 pandemic might have been had there been a robust global sewage-surveillance system in place. Researchers could have “immediately retroactively screened wastewater all around the planet” as soon as the virus’s sequence was released, Scarpino says. This screening could have led to a global list of places SARS-CoV-2 was already spreading, informing strategies to contain the virus even before clinical testing was widely available.
Scarpino argues that such a system would require major financial investment, national and scientific leaders who can take ownership of those projects and standards that make wastewater data more comparable across countries7.
The current COVID-19-testing community “came out of need and chaos”, says Megan Diamond, who works on wastewater surveillance at the Rockefeller Foundation in New York City. Global and regional institutions such as the World Health Organization, the European Union and the Africa Centres for Disease Control and Prevention might need to step up and offer guidance for testing, data sharing and standards, Diamond says.
Gawlik has worked on one such broad effort: the Global Consortium for Wastewater and Environmental Surveillance for Public Health, or GLOWACON, which was launched in Brussels in March. By recruiting more than 300 collaborators from around the world, including scientists, government officials and representatives of international organizations, to this consortium, he hopes to advance new methods for diagnosing health issues from the “dirty blood” of cities around the world.
The US Department of Health and Human Services (HHS) has issued a warning that hackers are attempting to target the helpdesks of hospitals in order to gain access to critical hospital systems.
The hackers have been observed contacting hospital IT help desks using local area code phone numbers and then pretending to be a hospital employee, providing the helpdesk with stolen identification.
The hackers then request that their device be set up to use the employee’s multi-factor authentication. Once they have access to the hospital’s internal systems, they are free to steal data and re-route transactions into their own bank accounts.
Hospital data and finances a honeypot for hackers
The Health Sector Cybersecurity Coordination Center (HC3) issued a warning for hospitals to be vigilant in the face of hackers using elaborate social engineering campaigns to gain access to hospital systems. The HC3 stated that the hackers “specifically targeted login information related to payer websites, where they then submitted a form to make ACH changes for payer accounts” in order to steal money.
“Once access has been gained to employee email accounts, they sent instructions to payment processors to divert legitimate payments to attacker-controlled U.S. bank accounts,” HC3 continued. “The funds were then transferred to overseas accounts. During the malicious campaign, the threat actor also registered a domain with a single letter variation of the target organization and created an account impersonating the target organization’s Chief Financial Officer (CFO).
While no threat actor has been formally identified as responsible for these attacks, HC3 issued a number of guidance points to IT help desks in order to avoid succumbing to such an attack: (PDF)
Require callbacks for employees requesting new device MFA enrollment or password resets using the number on file for the employee
Monitor ACH changes for suspicious activity and frequently revalidate users who have access to payer websites
Employees requesting MFA device enrollment, password resets, or ACH changes should report in person to the IT helpdesk
Where this is not possible, contact the employee supervisor for verification
Train helpdesk employees to identify social engineering techniques and spearphishing attempts
In 2010, Theresa Chaklos was diagnosed with chronic lymphocytic leukaemia — the first in a series of ailments that she has had to deal with since. She’d always been an independent person, living alone and supporting herself as a family-law facilitator in the Washington DC court system. But after illness hit, her independence turned into loneliness.
Loneliness, in turn, exacerbated Chaklos’s physical condition. “I dropped 15 pounds in less than a week because I wasn’t eating,” she says. “I was so miserable, I just would not get up.” Fortunately a co-worker convinced her to ask her friends to help out, and her mood began to lift. “It’s a great feeling” to know that other people are willing to show up, she says.
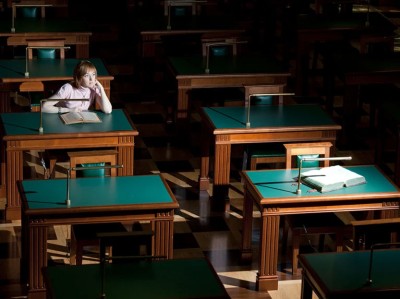
Many people can’t break out of a bout of loneliness so easily. And when acute loneliness becomes chronic, the health effects can be far-reaching. Chronic loneliness can be as detrimental as obesity, physical inactivity and smoking according to a report by Vivek Murthy, the US surgeon general. Depression, dementia, cardiovascular disease1 and even early death2 have all been linked to the condition. Worldwide, around one-quarter of adults feel very or fairly lonely, according to a 2023 poll conducted by the social-media firm Meta, the polling company Gallup and a group of academic advisers (see go.nature.com/48xhu3p). That same year, the World Health Organization launched a campaign to address loneliness, which it called a “pressing health threat”.
But why does feeling alone lead to poor health? Over the past few years, scientists have begun to reveal the neural mechanisms that cause the human body to unravel when social needs go unmet. The field “seems to be expanding quite significantly”, says cognitive neuroscientist Nathan Spreng at McGill University in Montreal, Canada. And although the picture is far from complete, early results suggest that loneliness might alter many aspects of the brain, from its volume to the connections between neurons.
Subjective and contagious
Loneliness is a slippery concept. It’s not the same as social isolation, which occurs when someone has few meaningful social relationships, although “they’re two sides of the same coin”, says old-age psychiatrist Andrew Sommerlad at University College London. Rather, loneliness is a person’s subjective experience of being unsatisfied with their social relationships.
The list of health conditions linked to loneliness is long and sobering1 (see ‘Loneliness and health’). Some of these make intuitive sense — people who feel lonely are often depressed, for example, sometimes to the point of being at risk of suicide. Other links are more surprising. Lonely people are at greater risk of high blood pressure and immune-system dysfunction compared with those who do not feel lonely, for example. There’s also a startling connection between loneliness and dementia, with one study reporting that people who feel lonely are 1.64 times more likely to develop this type of neurodegeneration than are those who do not3.
Source: The Cigna Group
A number of physiological effects, including the ability to sleep, increased stress-hormone levels and increased susceptibility to infections, could link loneliness with health problems. But the way in which these factors interact with one another makes it difficult to disentangle the effects of loneliness from the causes, cautions cognitive neuroscientist Livia Tomova at Cardiff University, UK. Do people’s brains start functioning differently when they become lonely, or do some people have differences in their brains that make them prone to loneliness? “We don’t really know which one is true,” she says.
Whatever the cause, loneliness seems to have the biggest effect on people who are in disadvantaged groups. In the United States, Black and Hispanic adults, as well as people who earn less than US$50,000 per year, have higher rates of loneliness than do other demographic groups by at least 10 percentage points, according to a 2021 survey by the Cigna Group, a US health-care and insurance company (see go.nature.com/43eakds). That’s not surprising because “loneliness, by definition, is an emotional distress that wants us to adapt our social situations”, says geriatrician and palliative-care physician Ashwin Kotwal at the University of California, San Francisco. Without financial resources, adapting is harder.
The COVID-19 pandemic might have exacerbated loneliness by forcing people to isolate for months or years, although “that data is still emerging”, Kotwal says. Older adults have long been thought of as the demographic most heavily affected by loneliness, and indeed it is a major problem faced by many of the older people that Kotwal works with. But the Cigna Group’s data suggest that loneliness is actually highest in young adults — 79% of those between the ages of 18 and 24 reported feeling lonely, compared with 41% of people aged 66 and older.
Loneliness eats at you
A growing amount of research is exploring what happens in the brain when people feel lonely. Lonely people tend to view the world differently from those who aren’t, says cognitive neuroscientist Laetitia Mwilambwe-Tshilobo at Princeton University in New Jersey. In a 2023 study, researchers asked participants to watch videos of people in a variety of situations — for example, playing sports or on a date — while inside an magnetic resonance imaging scanner4. People who did not report being lonely all had similar neural responses to each other, whereas the responses in people who felt lonely were all different — from the other group and from each other. The authors hypothesized that lonely people pay attention to different aspects of situations from non-lonely people, which causes those who feel lonely to perceive themselves as being different from their peers.
Feeling lonely in research? You’re not alone
This would mean that loneliness can feed back on itself, becoming worse over time. “It’s almost like a self-fulfilling prophecy,” Mwilambwe-Tshilobo says. “If you think that you’re lonely, you’re perceiving or interpreting your social world more negatively. And that makes you move further and further away.” Some studies have shown that this effect can spread through social networks, giving loneliness a contagious quality5.
Historically, staying close to others was probably a good survival strategy for humans. That’s why scientists think that temporary loneliness evolved — to motivate people to seek company, just as hunger and thirst evolved to motivate people to seek food and water.
In fact, the similarities between hunger and loneliness go right down to the physiological level. In a 2020 study, researchers deprived people of either food or social connections for ten hours. They then used brain imaging to identify areas that were activated by images of either food — such as a heaping plate of pasta — or social interactions, such as friends laughing together. Some of the activated regions were unique to images either of food or of people socializing, but a region in the midbrain known as the substantia nigra lit up when hungry people saw pictures of food and when people who felt lonely saw pictures of social interactions6. That’s “a key region for motivation — it’s known to be active whenever we want something”, says Tomova, who is an author on the study.
More links are emerging between loneliness and how the brain processes feelings of reward. In mice, loneliness sensitizes certain midbrain neurons to a neurotransmitter called dopamine7, which can also cause people to cave in to cravings, such as for food and drugs. Likewise, isolation might make humans more sensitive to rewards and more eager to seek them out. In 2023, Tomova and her colleagues published a preprint8 for a study in which they isolated adolescents from social contact for up to four hours. After isolation, participants were offered the chance to earn a monetary reward. The isolated participants agreed more quickly than did those who were not isolated, suggesting that isolation had made them more responsive to rewarding actions.
Loneliness and health
Although research on dopamine and loneliness is still emerging, scientists have also long recognized the connection between loneliness and another type of chemical signal — stress hormones called glucocorticoids. Humans need some level of glucocorticoids “to function; to wake up”, says neurophysiologist John-Ioannis Sotiropoulos at the National Centre for Scientific Research ‘Demokritos’ in Athens. But persistent loneliness leads to chronically high levels.
These chemicals could provide a link between loneliness and dementia. In a mouse model of Alzheimer’s disease, for example, glucocorticoids increased the levels of two proteins that are involved in the main hallmark of the condition, the protein plaques that tangle around neurons and interfere with memory and cognition9.
Stress is an extra assault on brains that are already wearing out as people get older, Mwilambwe-Tshilobo says, but she wants to see more research before committing to an opinion on exactly what part stress-related chemicals play in neurodegeneration. “It could accelerate the rate of ageing, but there hasn’t been work that explicitly looks at that,” she says.
Tomova says that although high levels of stress hormones probably contribute to dementia, it’s also likely that people who feel lonely miss out on the mental exercise that social interactions provide. And just as a muscle needs exercise to stay fit, so does the brain. In fact, loneliness has been associated with a smaller volume of grey matter in the brain10. “This is all hypothesis, really, at this stage,” Sommerlad says, but the idea is that socializing maintains neural connections that might otherwise be lost.
Turning inward
Researchers looking for the neural signature of loneliness have also found differences that could help to explain some of the correlations between loneliness and dementia. Previous research has suggested that there are changes in the connectivity between brain areas in people who feel lonely11. A 2020 study12 examined an area of the brain called the default network — so called because it’s active by default when a person isn’t engaged in a particular task and turns their attention inward — in older people who reported being lonely.
The hurt of loneliness and social isolation
Previous work had suggested that young people who feel lonely have high neural cross-talk between the default network and other networks associated with vision, attention and executive control13, possibly because they’re on high alert for social cues, says Spreng, one of the authors on the 2020 study of older people. But his team found the opposite in brain scans from the UK Biobank cohort of people aged 40 to 69. Loneliness weakened connections between the default network and the visual system and instead strengthened connections within the default network.
That could be because older people remedy loneliness by retreating into memories of past social experiences, Spreng says. In doing so, they strengthen the default network.
The default network is one of many networks in the brain that accrues damage during Alzheimer’s disease. Spreng and his colleagues are investigating whether strong default networks can indeed be linked to neurodegeneration — and if so, why. He wonders whether robust neural connections might allow pathologies to spread more readily in the network. The idea is far from proven, but it’s a plausible explanation and “an interesting hypothesis”, says cognitive neuroscientist Anastasia Benedyk at the Central Institute of Mental Health in Mannheim, Germany.
The study “lays the foundation for us to be able to test some hypotheses a little bit more empirically”, says Mwilambwe-Tshilobo, who was also involved in the work linking the default network with loneliness.
Finding solutions
Some remedies for loneliness will come as no surprise. Increasing access to social activities, for example by housing people in communities with common areas, can help, Sommerlad says. Some researchers are also finding ways to tap into the neural mechanisms underlying loneliness directly, through exercise, for instance.
Walking 4–5 kilometres over the course of an hour completely reversed feelings of low mood associated with loneliness in some people, Benedyk and her colleagues found14. What’s more, people with high connectivity in their default networks — the same area Spreng studied, which is also known to be affected by depression — were among those who benefited from exercise the most.
One possible explanation for this observation is that people with depression are “stuck in rumination” — a behaviour that draws heavily on the default network, Benedyk says. Exercise could force them to use other parts of their brain by interrupting neural processes that are associated with self-reflection and shifting activity to areas associated with physical activities — freeing them from a cycle of negative thoughts.
Exercising is also a great excuse to socialize. These days, Chaklos is retired, but she now leads the Boston branch of a US programme called ‘Walk with a Doc’, in which physicians invite community members to walk with them. At the group’s February walk, about 14 people chatted and strolled inside the Prudential Center mall in Boston, Massachusetts, where they could avoid New England’s winter weather. The activity “just uplifts a person’s mood”, Chaklos says. “Even if you’re still going back home to be by yourself, you don’t feel totally alone any more.”
Like most other corners of the tech world, Google sees AI powering the next innovations in health technology. The company’s annual The Check Up event expanded on its plans to add a personal health chatbot to the Fitbit app, expand Google Lens for better skin condition searches and use a version of its Gemini chatbot in the medical field.
One of the more intriguing of Google’s announcements on Tuesday was more detail about an experimental AI feature for Fitbit users, briefly teased last year. Fitbit Labs will let owners draw correlations and “connect the dots” from health data tracked using their wearable devices. A chatbot in the mobile app will let you ask questions in natural language and create personalized charts to learn about your health.
The company hasn’t yet gone into great depth about the Fitbit chatbot, but an example it published Tuesday shows a user asking about potential connections between activity and sleep. The Fitbit assistant answered that the user’s days with higher activity scores correlated with better sleep (while cautioning not to assume that’s the only reason).
The Fitbit generative AI tool will arrive later this year. Google says it will (at least initially) only be available to Fitbit Premium subscribers with Android devices enrolled in the Fitbit Labs program.
Google / Fitbit
The company sees Google Lens as filling some healthcare gaps where text-based searches fall short. It says a feature (introduced last year) that uses Lens to identify “visually similar matches from the web” for skin conditions is now available in over 150 countries. It can work even when you don’t know where to begin when describing a dermatological disorder.
In a similar light, Google has added new images and diagrams to its web results from reputable online sources to help you understand conditions like neck pain. Up next: The company sees the visual results powering its searches for more health conditions, including migraines, kidney stones and pneumonia. The visual search engine updates are expected to roll out over the next few months.
The company also mentioned that Fitbit and Google Research are partnering with health and wellness experts and other medical professionals to create a new AI model for health and wellness. The long-term goal is for the Gemini-powered large language model (LLM) to power its future AI features across Google’s various health offerings.
Last year, the Nature Index was broadened to include author affiliations from articles in more than 60 medical journals. The expansion, which covers all major disciplines and specialities in clinical medicine and surgery, offers new insights into global publishing trends in the health sciences. This is the first supplement to explore some of those trends.
The second noticeable data point is the dominance of Harvard University in the field. The institution, based in Cambridge, Massachusetts, has a Share (822) that is almost three times higher than the second-ranked institution, the US National Institutes of Health (290).
An extraordinary amount of money is invested in health-sciences research, but this hasn’t translated to a faster pipeline for new therapies. The increasing complexity of clinical trials is part of the problem, and something that researchers are hoping artificial intelligence can help to address. Others are rethinking how therapies are assessed in trials to make the results more meaningful. For example, could data impact people with Alzheimer’s and other progressive conditions by measuring how many ‘good years’ a medication can give, rather than comparing scores on cognitive tests?
Outside clinical trials, there are structural weaknesses in health-sciences research that need urgent attention, such as the lack of women in leadership positions. If institutions do not work harder to increase diversity at the top levels of academia, they risk damaging the talent pipeline and ultimately health outcomes for everyone.
Diversity in science is instrumental in achieving major breakthroughs. Without further accelerating gender parity and other types of diversity — including focusing on the needs of those in and working towards leadership roles — we will continue to lose valuable ground. At a time when academia faces some of its greatest workforce gaps in history, some of our brightest scholars are leaving institutions before reaching their full potential due to a lack of recognition.
Christina MangurianCredit: UCSF
We applaud changes that have been made for early-career researchers, with more women and historically excluded scholars entering research-training institutions now than ever before. But too often, we lose out on investments made by government funders and institutions in early-career researchers because the system was not built to increase the diversity of leaders as they move up the career ladder.
For 25 years, women have made up more than 40% of the medical student body in the United States, but less than 20% of department chairs in academic medicine. Without a major policy shift to accelerate the rate of diversification among leaders in the country, it will take 50 years for academic medicine to reach gender parity1. That’s way too long.
We must address this with urgency, as women’s perspectives and leadership are key in developing new therapies and improving representation in clinical trials. We need more role models for trainees and junior faculty. All of this leads to pipeline retention and more innovative discovery.
Claire D. BrindisCredit: Marco Sanchez, UCSF Documents and Media
So, what do we do? We must re-evaluate the way the entire scientific academic enterprise is set up to directly, and indirectly, create challenging climates for women, especially for women of colour. Below, we focus on the policies and procedures that would offer the highest yield in the context of the United States, but that have global relevance.
Elevate the status of gender equity on campus
Public policy value statements. Commitments by academic leaders to diversity measures must be backed by strong policies, protocols and actions directed at all career stages, but particularly focused on supporting emerging and senior women leaders. Organizations must hold leaders accountable for incidents of bias, discrimination and bullying and institute formal, tailored training to promote allyship for some, and active rehabilitation for others.
Confidential reporting. We need better reporting systems to ensure that researchers can highlight gender disparities without fear of retaliation. Ombudsman and whistleblower offices can be helpful, but in the United States, many of these are understaffed to meet the demand. There is also an urgent need to test which approaches are most effective at correcting behaviour.
Implement institutional family-friendly policies
Childbearing/rearing leave. In the United States, there have been gains for faculty members at some institutions and major gains nationally for trainees. But there is room to improve, such as provision of affordable, on-site childcare.
Lactation policies. Only 8% of US medical schools provide financial incentives to make up for clinical time lost while lactating in the first 12 months post-birth. Institutions should be leading the way in establishing policies that recognize the biological factors impacting careers.
Elder care and other informal care. A 2023 study2 found that close to half of female faculty are informal caregivers, and close to half are providing elder care as they reach mid-career. Given that institutions are competing to attract mid- or senior-level women, expansion of paid leave policies to include elder care is warranted.
Nature Index 2024 Health sciences
Formalize equitable distribution of resources and access to opportunities
Compensation. Institutions should regularly perform salary reviews as a means of correcting disparities, especially as it pertains to women of colour. Leaders should also regularly review starting salaries, distribution of endowed chairs, salary increases that are far above the norm and recruitment and retention packages.
Sponsorship. Mentoring and sponsorship roles are increasingly recognized, but more oversight is needed. Behind closed doors is where decisions are made as to who gains access to crucial leadership opportunities; making the invisible visible is key to assuring greater institutional equity.
Focus on faculty promotion and retention
Resources. Offering equitable start-up packages and discretionary funds for new faculty members as well as compensation for dedicated mentors for historically excluded early career researchers can create a supportive professional environment. Such resources are important to offset the time requirements placed on excluded groups who are frequently asked to serve on campus and department committees to meet diversity metrics.
Peer support. Community affinity groups facilitate knowledge exchange needed for career advancement, as well as ‘real time’ support for faculty members. They are easy to set up and yield high returns for participants.
A multi-pronged approach is needed to accelerate gender parity in academic medicine leadership. Rather than continue to attribute disparities to individual ‘failures’, institutions must recognize that structural and organizational interventions can make transformational change.
If you’re like me, you might never have heard of continuous glucose monitors (CGMs) until the last few months, if at all. However, if your online presence has found its way on to any health or wellness algorithms, you’ve almost certainly encountered at least one or two advertisements or endorsements for the technology.
That’s because these smart glucose sensors are being touted by manufacturers and lifestyle brands as the key to unlocking and improving metabolic health, despite having been invented primarily to provide diabetes patients with real-time glucose readings.
Graph showing the worldwide search interest for CGMs increasing over the last year (Source: Google) (Image credit: Future / Canva)
But what is metabolic health, and does the information generated by these devices provide any insight that can provably help non-diabetic users? These are the questions I sought to answer when I began my journey trialing CGMs this year.
So, in addition to testing out Lingo by Abbott and the Zoe diet, I’ve spoken with nutritionists, diabetes experts and CGM gurus to find out what all the fuss is about.
What is a CGM, and who’s it for?
CGMs pack some pretty fascinating technology. Once applied, they look pretty nondescript; just a white disc stuck onto your arm and rarely larger than 1.4-inches / 3.5cm in diameter. Under the hood, however, there’s a lot going on.
CGMs insert a subcutaneous (under the skin at the layer closest to your muscle) sensor, using an algorithm to estimate blood glucose concentration based on the levels they find in the interstitial fluid (found in the spaces between cells). They do it in almost real-time, with a delay of just 15-30 minutes depending on the sensor. This data is then transmitted to a companion app and translated into a glucose reading to show how your body responds to recently eaten foods.
I spoke with Dr. Mark J. O’Connor, Assistant Professor of Medicine and practicing endocrinologist, to learn more about how these devices are used in a clinical setting.
Dr. O’Connor is an Assistant Professor of Medicine at the UMass Chan Medical School in Worcester, Massachusetts, and a practicing endocrinologist at UMass Memorial Health Care System, particularly in the UMass Diabetes Center of Excellence. He’s also conducted a small research study on the utility of using CGMs to help diabetes patients in emergency departments.
He explains: “A CGM is a useful tool for people with diabetes, because it gives them a lot more insight into their blood sugar levels, and it gives us as healthcare providers more insight so that we can make the best recommendations.
“It also helps people make better decisions about exercise, food, and other factors that affect blood sugar levels. For many people with diabetes, it’s a Godsend.”
The technology has come a long way since 1999, when it gained Food and Drug Association approval for clinical use in the US. Abbott, one of three US companies manufacturing the majority of CGMs worldwide, is one of the first to take its technology into the consumer space; its consumer offering, Lingo, arrived in the UK in January, and pending FDA clearance is set to be released in the US later this year.
I spoke with Olivier Ropars, Division VP of Lingo Biowearables, about the company’s expansion into direct-to-consumer CGMs.
Olivier Ropars
Ropars joined Abbott in 2022 to run Lingo, Abbott’s consumer Biowearables division, where he is currently overseeing the growth of the product as it comes to market in various regions. He previously held positions at eBay, StubHub and McKinsey.
The key benefit to direct-to-consumer CGMs, says Ropars, lies in understanding your metabolic health – which, broadly speaking, is the absence of metabolic disorders, including conditions such as type 1 diabetes, obesity, and inflammatory bowel diseases. They can also be vital tools in measuring the long-term effects of hypoglycemia (low blood glucose) and hyperglycemia (high glucose levels).
As Ropar explains, a series of studies conducted by Abbott employees and consultants found post-meal glucose spikes correlate to sleep and mental health difficulties and increased hunger. More worryingly, they were also associated with the development of type 2 diabetes and an “increased risk of seven out of the 10 leading causes of death in the US; that’s expected to be the same in the UK.” These include cardiovascular disease, liver failure, kidney failure, and increased risk of developing Alzheimer’s.
(Image credit: Shutterstock / Dragoljub Bankovic)
CGMs: Fad or fact
“The current healthcare system is entirely focused on curing diseases or trying to catch diseases early. There’s very little focus on disease prevention,” says Ropars, citing findings that health trackers such as pedometers have an “overwhelmingly positive” impact on people’s lifestyles. CGMs, he argues, will have the same effect.
Ropars says three groups of people have been particularly receptive to Lingo. The first is people, particularly athletes, looking to optimize their health and performance. These bio-hackers are a core demographic across many CGM offerings; the recently shuttered Supersapiens CGM-based platform (which also used Abbott sensors) enticed users with the promise they’d “never bonk again”, referring to the exercise-induced hypoglycemia endurance athletes can experience when they haven’t eaten enough carbohydrates. Indeed, early studies have shown CGMs might be useful for athletes in determining ideal carbohydrate intake – but as of yet, this isn’t proven.
The second and third groups are more general; people wanting to resolve age- or health-related issues who haven’t seen success in one-size-fits-all solutions; and those with a family history of disease wanting to monitor health and take preventative measures.
Many brands, such as Zoe in the UK and Super Sapiens in the US use Abbott’s CGMs paired with their own proprietary platforms for data analysis and lifestyle guidance. (Image credit: Shutterstock / Jeniffer Fontan)
O’Connor can likewise see the benefits: “To me, it does make sense that giving people access to more information would be helpful. To see the effect on your blood sugar of routine exercise or a healthy diet is positive reinforcement to continue to make healthy behavioral changes.” A small study funded by Dexcom, another major CGM manufacturer, supports this, seeing a small group of people generally improve their lifestyle after using a CGM.
Lauren Johnson Reynolds, AKA the London Wellness Coach, is a homeopath, nutritionist, and health coach with a special interest in hormone balance following her own experience with polycystic ovarian syndrome (PCOS). Early studies have shown a correlation between glucose tolerance, diabetes, and PCOS, which is why Reynolds tried out CGMs after giving birth led her HBA1-C to elevate to a near pre-diabetic range.
“There were certain foods and combinations that I felt wouldn’t cause any issues, but were spiking my blood sugar quite badly,” she says. “It was very eye-opening, and I became very aware of how stress impacted my blood sugar.”
Lauren Johnson Reynolds
Following a series of health difficulties relating to stress and PCOS, Reynolds turned to homeopathic solutions to relieve her symptoms, beginning a journey of healing and self-understanding that culminated in her studying an integrated Homeopathy and Nutritional therapy course. Now, she shares her knowledge, passion and holistic approach to wellness as a health coach.
A double-edged needle
While there’s plenty of buzz around the potential for CGMs, there’s perhaps not significant enough proof to convince some practitioners. Katherine Metzelaar, MSN, RDN, CD, founder and CEO of Bravespace Nutrition, is one of many concerned parties. “There’s this general desire to want to know what’s going on inside of our bodies – but it’s not as simple as that.
“We have yet to hear about any positive impacts of continuous glucose monitoring outside of the management of diabetes, and I think they cause more harm than good.”
Katherine Metzelaar, MSN, RDN, CD
Passionate about helping people battling disordered eating, Katherine Metzelaar’s approach is to help cultivate a positive food and body relationship by creating a weight-inclusive space and educating clients on the impacts of diet culture. Her specialism is in eating disorder recovery, body image concerns, and weight-inclusive nutrition therapy, which she practices using the HAES (health at every size) approach.
Metzelaar specializes in disordered eating and food positivity, and fears CGMs are another chapter in a legacy of illusory diet and wellness fads that contribute to an ineffective approach to health.
“It could lead to oversimplifying nutrition, increased stress and anxiety around food, and unnecessary restriction or inaccurate and inadequate advice around what to do with that information,” she says. “My recommendation is usually not to do it. Even for clients I work with that have diabetes, it leads to them feeling anxious when they see their glucose spike.”
She’s also broadly unconvinced by the usefulness of the data provided, especially the difficulty in parsing what specifically might have elevated glucose levels when eating different foods.
Despite her own positive experience, Reynolds has similar concerns about the broader use of CGMs. “I recommend them to a few clients but not the majority… When you step back and look at it, it’s quite extreme, but we’re so used to monitoring our sleep and our recovery, it’s become very normalized.”
Lingo by Abbott provides real-time insight into blood glucose levels, presenting spikes as “Lingo counts” and encouraging users to stay below a target each day. The target is based on your health data; factors such as age, gender and weight. (Image credit: Future)
“Modern society has lost track of hunger signals and thirst signals. We’re told to drink eight glasses of water a day and eat three meals and two snacks, and so that’s what we do. It’s taking away from that mind-body connection. So, although I think they are extremely useful for people who have blood-sugar issues, have a condition like PCOS, or want to try CGMs for a short amount of time, for the average person I don’t think it’s necessary.”
Metzelaar also has concerns about the self-led nature of many CGM platforms. “To my understanding, there’s no oversight from a doctor or a dietitian to interpret that information and add clarity to it.” This, she says, could lead users to change their behaviors based on what could simply be the normal curve of what happens during digestion.
I tried two different CGMs as part of my research for this article; Zoe Health and Lingo. While I don’t have any metabolic health diagnoses, I’ve had a lot of digestive and stress-related issues in recent months – but for me, this technology is still perhaps a little extreme. (Image credit: Future)
Knowledge is power – until it’s not
As of right now, there are numerous consumer-based studies underway, including large-scale efforts being conducted by CGM platforms including Levels and Signos. In the UK, Zoe Health combines gut microbiome, blood sample, and bowel movement data with its CGM readings, the results of which can be discussed with a Zoe nutritionist. Clearly, there’s plenty of confidence from these providers that there’s something in this CGM craze worth fighting for.
That’s certainly the resounding take of Ropars, who says we’re only just beginning to unlock the potential of CGMs: “It’s not like buying a diet book; that may not work for everyone. A CGM provides personalized information, so you can make the adjustments that matter the most for you.”
So, are CGMs a fad or the future of wellbeing? As of right now, they don’t definitively support non-diabetics to improve their lifestyle, nor can studies fully demonstrate the biomarkers they track have a measurable impact on long-term health and wellbeing.
Still, the appetite for the technology and the research being conducted into metabolic health, blood glucose, and the relationship with long-term health means, for better or worse, we’re likely going to be seeing a lot more about CGMs in the coming years.
Powerful new health and wellness apps take advantage of visionOS’s “infinite canvas” to use spatial experiences to improve patient outcomes in clinical settings and at home, Apple said Monday. It seems that Vision Pro health apps are changing medical care.
“We’re thrilled to see the incredible apps that developers across the healthcare community are bringing to Apple Vision Pro,” said Susan Prescott, Apple’s vice president of Worldwide Developer Relations. “The imagination and drive of our developers, combined with the technical capabilities of visionOS, are igniting new possibilities for physicians, frontline workers, and even students, and we can’t wait to see what’s to come.”
visionOS health apps benefit users through spatial experiences
Accordingly, Apple pointed out that medical institutions and developers have worked with products like iPad and iPhone for a long time. Apple gear has helped improve patient outcomes, increase efficiency, save money and supercharge research. Now it’s Vision Pro’s turn.
“Vision Pro seamlessly blends digital content with the physical world, unlocking powerful spatial experiences in an infinite canvas,” Apple said. “And with the unique capabilities of visionOS, healthcare developers are creating new apps that were not previously possible. [They] transform areas such as clinical education, surgical planning, training, medical imaging, behavioral health and more.”
In support of the premise, the iPhone giant listed some choice examples of healthcare and wellness apps.
Aiding behavioral health and wellness
Cedars-Sinai’s Xaia app (pictured above; watch a video demo) uses Vision Pro to support patients’ mental health. The app’s “trained digital avatar offers patients AI-enabled, conversational mental health support in relaxing spatial environments where they can also do deep breathing exercises and meditation.” The patient could be at home or somewhere like a beach. And privacy remains intact, as the app requires no patient information.
“Apple Vision Pro’s stunning display offers a gateway into a world of immersive, interactive behavioral health support — a quantum leap beyond previous technologies,” said Brennan Spiegel, MD, MSHS, professor of medicine, director of Health Services Research, and director of the master’s degree program in Health Delivery Science at Cedars-Sinai.
“With Xaia, we leverage every pixel of that remarkable resolution and the full spectrum of vivid colors to craft a form of immersive therapy that’s engaging and deeply personal,” he added. “With this remarkable device, our team was able to completely reimagine how spatial computing can support behavioral health and overall wellbeing in ways never before possible.”
And you can explore other behavioral health and wellness apps:
The Mindfulness app on Vision Pro creates calm, immersive environments for users.
TRIPP delivers illuminating visuals and Spatial Audio for guided breathing exercises and sleep experience.
Healium helps Vision Pro users “relax and build resilience by creating stress-reducing memories of nature-based escapes.”
Odio uses Spatial Audio and intuitive gestures to display 3D images for focus, relaxation or peaceful sleep.
Surgical planning and education with Vision Pro health apps
Apple pointed out Stryker’s new myMako app for the company’s Mako SmartRobotics hip and knee replacement surgeries. The app helps surgeons use Vision Pro and iPhone to extend their experience in and beyond the operating room for better surgical outcomes. It helps surgeons prepare by visualizing and reviewing patients’ Mako surgical plans through immersive visuals.
“The myMako app for Apple Vision Pro allows surgeons the ability to access intricate surgical plan details and insights at their fingertips in a 3D-native, intuitive, and dynamic way. This level of insight — anytime, anywhere — was previously not possible,” said Robert Cohen, Stryker’s president of Digital, Robotics, and Enabling Technologies.
“With Apple Vision Pro, Stryker’s market-leading enabling technologies such as Mako SmartRobotics have the exciting potential to transform the way surgeons think about preoperative planning and the intraoperative experience, all consistent with Stryker’s mission to make healthcare better.”
Virtual environments for training
Boston Children’s Hospital created CyranoHealth, an app that offers immersive, comprehensive training on new medical equipment for frontline workers. Photo: Apple
In addition, Apple cited Boston Children’s Hospital’s CyranoHealth app. Its comprehensive learning experience in a virtual environment helps with onboarding and training of clinicians. This is especially helpful in prepping them for real-world use of new medical equipment.
“CyranoHealth utilizes spatial computing to revolutionize the training of healthcare professionals, offering immersive, lifelike simulations to enhance learning and combat burnout. The app represents a significant leap forward in healthcare training, blending technology and medicine to create a future-ready workforce,” said John Brownstein, Ph.D., Boston Children’s chief innovation officer.
And you can explore other surgical planning and education apps:
Fundamental Surgery delivers surgical training through spatial computing.
CollaboratOR 3D by KARL STORZ enhances surgical learning opportunities.
Elsevier’s Complete HeartX “delves into … the human body to create a realistic and engaging learning environment.”
Insight Heart helps users understand the human heart. With ARKit, they can scan physical surroundings and visualize 3D hearts using CT data.
Interactive holograms
Siemens Healthineers’ Cinematic Reality app for Vision Pro lets clinicians and patients see immersive, interactive holograms of the human body taken from medical scans.
So here’s Apple’s description of how it works:
Using Metal and the power of the M2 processor, the app integrates advanced path-tracing technology, simulating light interactions with virtual objects to deliver breathtakingly realistic lighting and reflections.
“Cinematic Reality gives people the opportunity to immerse themselves in a world of photorealistic renderings of the human anatomy,” said Christian Zapf, of Siemens Healthineers. “Apple Vision Pro perfectly presents that three-dimensional experience, combined with great flexibility and standalone use. We see great potential for the technology for clinical as well as educational purposes.”
Vision Pro health apps: Collaborative medical histories
Epic Spatial Computing Concept allows physicians to experience charting, secure chat, and in-basket workflows with Apple Vision Pro using gestures. Photo: Apple
And another good example of an enhanced health app involves all-important medical records.
Epic Systems’ Epic Spatial Computing Concept for Vision Pro helps healthcare workers in various ways. They can “easily complete charting, review labs, communicate using secure chat, and complete in-basket workflows through intuitive gestures.”
“Creating the first electronic health record experience for spatial computing was an exciting project for our developers,” said Seth Howard, Epic’s senior VP of R&D. “With Apple Vision Pro, clinicians will be able to interact with their patients’ health information in new, immersive ways. We welcome ideas from the physician community about how this technology can expand the future of healthcare delivery.”
And you can explore other productivity and collaboration apps:
Visage Ease VP supports immersive spatial experiences for diagnostic imaging and multimedia. UC San Diego Health became the first health system to pilot the technology t0 improve patient care.
Falcon Vue unleashes the power of spatial medical imaging viewing.
Medivis brings SurgicalAR Vision to Apple Vision Pro, enhancing medical imaging to support surgical precision.
Long-term use of antiretroviral drugs can cause abnormal fat accumulation in people with HIV.Credit: Jose Calvo/SPL
People with HIV are the latest group to benefit from the new generation of anti-obesity drugs. If early data about the treatments’ effects are confirmed, the drugs could become key to controlling the metabolic problems often caused by anti-HIV medications.
Studies presented last week at the Conference on Retroviruses and Opportunistic Infections in Denver, Colorado, suggest that the anti-obesity drug semaglutide not only helps people with HIV to lose weight but also reduces certain conditions associated with fat accumulation that are especially common in people infected with the virus.
Game-changing obesity drugs go mainstream: what scientists are learning
The number of people who are overweight or have obesity is increasing among those with HIV, driving interest among both affected individuals and medical providers in medications such as semaglutide, says Daniel Lee, a physician at the University of California San Diego Medical Center. At his clinic, which treats people with metabolic complications of HIV therapies, around 20% of patients already receive semaglutide or other drugs of the same class.
“For the most part, we’ve had very good experiences with these medications,” Lee says. But, so far, few studies have looked at the effect of the blockbuster anti-obesity drugs on people with HIV.
Unwanted side effects
Although the increasing incidence of obesity in people with HIV is similar to the trend in the general population, certain antiretroviral medications used to suppress HIV could contribute further to weight gain and weight-related conditions in these individuals1,2.
Semaglutide, marketed as Wegovy for obesity and Ozempic for diabetes, mimics a hormone called glucagon-like peptide 1, which helps to lower blood sugar levels and control appetite. In people who are overweight or have obesity, the drug promotes substantial weight loss3.
In a talk on 4 March, researchers at the Centers for AIDS Research Network of Integrated Clinical Systems, a group of HIV clinics across the United States, described their analysis of semaglutide use by 222 individuals receiving HIV care. The drug was associated with an average weight loss of 6.5 kilograms in around one year, or 5.7% of initial body weight.
Helping a fatty liver
Antiretroviral therapies have also been associated with abnormal fat accumulation. One condition affecting 30–40% of people with HIV is metabolic dysfunction-associated steatotic liver disease, which is characterized by the build-up of fat in the liver. As the condition progresses, it can result in liver failure and cardiovascular disease. “We do know that people with HIV have a more aggressive form of fatty liver disease,” says Jordan Lake, an infectious-disease physician at the University of Texas Health Science Center at Houston. But there is currently no approved medication to treat the condition.
Fatty liver disease: turning the tide
She and her colleagues evaluated the use of a weekly injection of semaglutide for around six months in people with both HIV and metabolic dysfunction-associated steatotic liver disease. The results, presented on 5 March, demonstrated that 29% of participants had a complete resolution of the liver disease. “What we saw were really great clinically significant reductions in liver fat even over that short period of time,” Lake said at the conference.
But data from the same study show that participants taking semaglutide lost muscle volume, an effect also observed in other people taking the drug. Individuals who were 60 years of age or older were affected the most. Lee notes that older individuals with HIV are especially vulnerable to semaglutide-linked muscle loss and should be followed closely by health-care providers.
Taming inflammation
Another talk at the conference examined the use of semaglutide for a condition called lipohypertrophy in people with HIV. Characterized by the accumulation of abdominal fat, it “is associated with increased inflammation and carries an increased cardiometabolic risk”, says Allison Eckard, an infectious-disease paediatrician at the Medical University of South Carolina in Charleston. “We have currently few treatments and those treatments often show ineffective response rates.”
Obesity drugs have another superpower: taming inflammation
In an earlier clinical trial, Eckard and her colleagues scanned the bodies of people with HIV and lipohypertrophy and found that semaglutide helped to reduce abdominal fat. They had presented results from that study in October at IDWeek, a meeting of infectious-disease specialists and epidemiologists in Boston, Massachusetts. And at the conference in Denver, the team showed that a blood marker of inflammation called C-reactive protein fell by almost 40% in study participants who took semaglutide compared with those who did not.
That could be an important effect, because even well-controlled HIV leads to a chronic state of inflammation, Lee says. And, he says, “if there’s increased inflammation, it can lead to end-organ disease of all sorts, including certainly cardiovascular outcomes, but also liver, kidney, brain, cognitive function, you name it”.