The way that users get information from the web has evolved over the years. People used to rely on news sites and Google to keep abreast of what was going on in the world, but then Twitter arrived and cemented itself as an alternative (and often inaccurate) source of news. Although it’s facing the threat of being banned in the US, TikTok has become a major source of information for younger users, and AI chatbots have really come into their own as a valuable tool for delivering tailored, instant information.
The rise of voice-activated AI assistants like Amazon‘s Alexa and Google Assistant has also revolutionized the way we access information, allowing users to simply ask for what they want to know, rather than having to search for it manually. However, with this evolution comes the responsibility of discerning reliable sources from misinformation, a skill that is becoming increasingly important in the AI age.
Recent surveys by Applause and Forrester indicate a significant shift in consumer behavior, with users increasingly favoring AI chatbots over traditional search engines for both research and basic queries.
Similar findings
Applause‘s 2024 Generative AI Survey reveals that 91% of respondents use chatbots for research, and 81% prefer them over search engines for basic queries. However, as is perhaps to be expected, concerns about data privacy, bias, and performance persist.
Applause found ChatGPT is the most popular chatbot, used by 91% of users, ahead of Google Gemini (63%) and Microsoft Copilot (55%). Despite worries about providing private information to chatbots, with 89% of respondents expressing concern, the practical applications of Gen AI are now widely acknowledged. However, only 19% of users believe that chatbots understand their prompts every time, indicating room for improvement.
Forrester‘s State of Consumer Usage of Generative AI 2024 echoes these findings, noting that GenAI has made AI more visible in consumers’ daily lives. While companies race to incorporate AI, consumer adoption is still in its infancy due to concerns about its ethical implications. The report also highlights the demographic differences in GenAI adoption, with younger, male, and more highly educated consumers more likely to have used the technology. The report states that almost half of Millennial and Gen Z adults in the US, UK and France have used GenAI, compared with only 12% of Baby Boomers.
Forrester also found 34% of US consumers used GenAI, compared to 27% in the UK and 25% in France.
Sign up to the TechRadar Pro newsletter to get all the top news, opinion, features and guidance your business needs to succeed!
Work still needed
Despite widespread concerns, the benefit of GenAI is widely recognized. Among online adults who had heard of GenAI, 50% agreed that it would make it easier to find information online. However, 45% agreed that GenAI posed a serious threat to society, indicating a split in consumer attitudes towards the technology.
The surveys reveal that the golden era of search engines might be coming to an end, as consumers increasingly turn towards AI chatbots for their information needs. However, as Chris Sheehan, SVP Strategic Accounts and AI at Applause sums up, “Chatbots are getting better at dealing with toxicity, bias and inaccuracy – however, concerns still remain. Not surprisingly, switching between chatbots to accomplish different tasks is common, while multimodal capabilities are now table stakes. To gain further adoption, chatbots need to continue to train models on quality data in specific domains and thoroughly test across a diverse user base to drive down toxicity and inaccuracy.”
South Korean science minister Lee Jong-ho and European commissioner for research Iliana Ivanova celebrate South Korea joining Horizon Europe in March. Viewing research through a security lens makes it harder for other non-EU countries to follow.Credit: HANDOUT/EPA-EFE/Shutterstock
Last month, the European Commission published a ‘course correction’ for its Horizon Europe research fund, which is worth around US$100 billion over seven years, from 2021 to 2027. It’s not easy to make major alterations at the mid-way point of such a large enterprise, whose two predecessors funded 1.5 million collaborations across 150 countries. But the European Union has made substantial changes in the fund’s latest strategic plan that researchers need to be aware of.
One of the most important is a phrase now peppered throughout the document: open strategic autonomy.
This political concept means that the EU will strengthen its self-sufficiency while remaining open to cooperation with other regions. The term is not new — in Horizon Europe’s first strategic plan (for 2021–24), open strategic autonomy was one of four priority areas for funded projects, alongside the green transition, the digital transition and building a more resilient, competitive, inclusive and democratic Europe.
Horizon Europe turmoil changed the lives of these five scientists
The EU has reduced these four priorities to three — and open strategic autonomy has been upgraded. It is now an overarching theme for all research funded by Horizon Europe from 2025 to the end of 2027. Barring a sudden outbreak of world peace, this mode of thinking and action is expected to influence — if not dominate — the next iteration of Horizon Europe, called FP10, which will start in 2028.
This change of priorities is concerning researchers. The European Research Council (ERC), which funds investigator-led research and is part of Horizon Europe, issued a statement at the end of January, saying: “The ERC’s independence and autonomy must be protected under FP10.”
But for now, just as a tanker cannot be turned around at full speed, Horizon Europe retains key elements of the original plan. The EU wants to maintain its climate funding (35% of the total Horizon Europe budget) and increase biodiversity funding to 10% of the budget, which are both welcome decisions. It is also committed to the idea of moonshot-style missions: specific goal-oriented funds to tackle urgent global challenges, such as improving soil health and establishing carbon-neutral cities. It plans to meaningfully integrate social-sciences and humanities researchers into collaborations — not just include them as afterthoughts — and to improve diversity and equity. And it is continuing to reach beyond its borders.
War shattered Ukrainian science — its rebirth is now taking shape
Last week, it was announced that South Korea’s researchers will be able to participate in EU-funded projects related to global challenges. Last November, Canada also joined the programme. And New Zealand before that. The United Kingdom’s researchers are also back, after a gap of nearly four years after Brexit. These are, broadly speaking, all representative democracies with which EU countries have defence- and security-cooperation agreements. The principle of open strategic autonomy will make it more difficult to cooperate with countries for which this is not the case.
The EU is obviously responding to the world-changing events of the past decade. When discussions about the first iteration of Horizon Europe were beginning, wars, pandemics and the election of populist leaders mostly seemed to be twentieth-century concerns. As the EU — and its international partners, too — responded to levels of instability that few were expecting, heavier emphasis on a research agenda to strengthen supply chains, ensure resilience of essential infrastructure and establish more manufacturing at or closer to home is understandable.
But a security mindset cannot be baked into what is fundamentally an open and autonomous research cooperation fund. In addition to sharing research and cooperating in the development of new technologies, Horizon Europe — originally called the Framework Programme — was created to re-establish trust between Europe’s nations in the second half of the twentieth century. It was part of a larger effort to prevent them from going to war with each other.
Strategic plans have to remain flexible. Circumstances change, and it’s important to be able to make adjustments when that happens. But making open strategic autonomy a theme for all EU funding is neither sensible nor desirable.
Last September, while completing a grant application, I faltered at a section labelled ‘summary of progress’. This section, written in a narrative style, was meant to tell reviewers about who I was and why I should be funded. Among other things, it needed to outline any family leave I’d taken; to spell out why my budget was reasonable, given my past funding; and to include any broad ‘activities, contributions and impacts’ that would support the application.
How could I sensibly combine an acknowledgement of two maternity leaves with a description of my engagement with open science and discuss why I was worthy of the funding I’d requested? There was no indication of the criteria reviewers would use to evaluate what I wrote. I was at a loss.
Bring PhD assessment into the twenty-first century
When my application was rejected in January, the reviewers didn’t comment on my narrative summary. Yet they did mention my publication record, part of the conventional academic CV that I was also required to submit. So I’m still none the wiser as to how the summary was judged — or if it was considered at all.
As co-chair of the Declaration On Research Assessment (DORA) — a global initiative that aims to improve how research is evaluated — I firmly believe in using narrative reflections for job applications, promotions and funding. Narratives make space for broad research impacts, from diversity, equity and inclusion efforts to educational outreach, which are hard to include in typical CVs. But I hear stories like mine time and again. The academic community is attempting, in good faith, to move away from narrow assessment metrics such as publications in high-impact journals. But institutes are struggling to create workable narrative assessments, and researchers struggling to write them.
The problem arises because new research assessment systems are not being planned and implemented properly. This must change. Researchers need explicit evaluation criteria that help them to write narratives by spelling out how different aspects of the text will be weighted and judged.
Research communities must be involved in designing these criteria. All too often, researchers tell me about assessment systems being imposed from the top down, with no consultation. This risks these new systems being no better than those they are replacing.
How to boost your research: take a sabbatical in policy
Assessments should be mission-driven and open to change over time. For example, if an institute wants to increase awareness and implementation of open science, its assessments of which researchers should be promoted could reward those who have undertaken relevant training or implemented practices such as data sharing. As open science becomes more mainstream, assessments could reduce the weight given to such practices.
The value of different research outputs will vary between fields, institutes and countries. Funding bodies in Canada, where I work, might favour grants that prioritize Indigenous engagement and perspectives in research — a key focus of diversity, equity and inclusion efforts in the Canadian scientific community. But the same will not apply in all countries.
Organizations must understand that reform can’t be done well on the cheap. They should invest in implementation scientists, who are trained to investigate the factors that stop new initiatives succeeding and find ways to overcome them. These experts can help to get input from the research community, and to bring broad perspectives together into a coherent assessment framework.
Some might argue that it would be better for cash-strapped research organizations to rework existing assessments to suit their needs rather than spend money on experts to develop a new one. Yes, sharing resources and experiences is often useful. But because each research community is unique, copying a template is unlikely to produce a useful assessment. DORA is creating tools to help. One is Reformscape (see go.nature.com/4ab8aky) — an organized database of mini case studies that highlight progress in research reform, including policies and sample CVs that can be adapted for use in fresh settings. This will allow institutions to build on existing successes.
The postdoc experience is broken. Funders such as the NIH must help to reimagine it
Crucially, implementation scientists are also well placed to audit how a new system is doing, and to make iterative changes. No research evaluation system will work perfectly at first — organizations must commit sustained resources to monitoring and improving it.
The Luxembourg National Research Fund (FNR) shows the value of this iterative approach. In 2021, it began requesting a narrative CV for funding applications, rather than a CV made up of the usual list of affiliations and publications. Since then, it has been studying how well this system works. It has had mostly positive feedback, but researchers in some fields are less satisfied, and there is evidence that institutes aren’t providing all researchers with the guidance they need to complete the narrative CV. In response, the FNR is now investigating how to adapt the CV to better serve its communities.
Each institution has its own work to do, if academia is truly to reform research assessment. Those institutions that drag their feet are sending a message that they are prepared to continue supporting a flawed system that wastes research time and investment.
Competing Interests
K.C. is the co-chair of DORA (Declaration On Research Assessment) — this in an unpaid role.
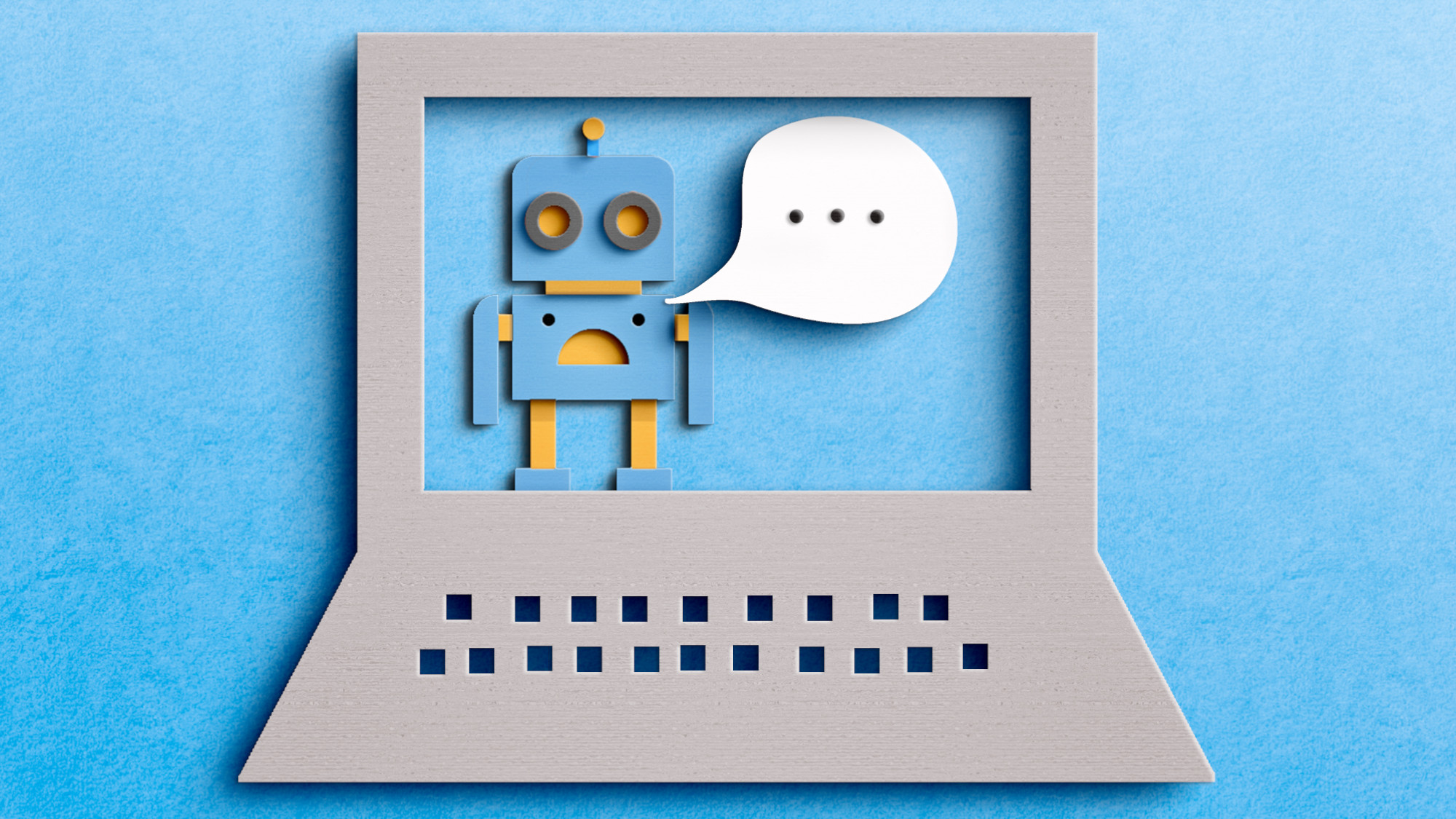
When Lisa McCorkell got COVID-19 in March 2020, her symptoms were mild. Her physicians told her to isolate from others and that she would recover in a few weeks. But the weeks stretched into months and McCorkell, who was working on a master’s degree in public policy at the University of California, Berkeley, started having debilitating and bewildering symptoms: fatigue, dizziness and shortness of breath. Previously an avid runner, McCorkell found her heart racing from simple efforts.
She struggled to find an explanation, and soon realized that her physicians didn’t know any more about her condition than she did. To complicate matters, the limited availability of high-quality testing for the coronavirus SARS-CoV-2 in the early days of the pandemic left many of her doctors wondering whether her symptoms were really due to COVID-19 at all. “I didn’t have health-care providers that took me seriously,” McCorkell says. “That largely pushed me out of the health-care system.”
McCorkell turned instead to those who were experiencing the same puzzling symptoms and frustrations, joining a support group for people with what would eventually be called long COVID. As they compared notes, McCorkell and a handful of others — many of whom had research experience — realized that the information they were sharing might be helpful not only for those with long COVID, but also for those looking to study the condition. So, they founded a non-profit organization, called the Patient-Led Research Collaborative (PLRC), to design, provide advice on and even fund basic and clinical research into long COVID and other chronic illnesses.
Four years on: the career costs for scientists battling long COVID
A survey run by the group and published in 2021 catalogued the more than 200 symptoms experienced by people with the condition (H. E. Davis et al. eClinicalMedicine38, 101019; 2021). It is seen by some as putting long COVID on the map. “They really jump-started the interest,” says Lucinda Bateman, a physician in Salt Lake City, Utah, who specializes in treating people who have long COVID and related conditions. “That was really a point from where more broad awareness arose.”
In the past few years, this study and similar patient-led efforts have helped to shape research programmes on long COVID and kick off some early clinical trials of therapies that might otherwise have gone unexplored. Many patient advocates see the efforts as crucial. They also think the results are more helpful for advancing the understanding of long COVID than the current findings from programmes funded by the US$1.15-billion RECOVER initiative led by the US National Institutes of Health (NIH). People with long COVID and their advocates have criticized the initiative for not always listening to the needs of people with long COVID.
Getting involved in research is challenging, given the symptoms of long COVID, but many patient advocates say they have no choice. “They’ve got you over a barrel,” says Margaret O’Hara, who coordinates patient involvement in research for a National Health Service hospital trust in England. O’Hara is on medical leave owing to long COVID. Referring to the research, she says: “You have to do it, because you are the one who is going to suffer for it if you don’t, but at the same time, you’re in bed sick.”
A plethora of symptoms
The PLRC’s survey of long COVID symptoms was the first major research study of the condition. The premise was simple enough: authors surveyed almost 3,800 people in 56 countries, many of whom were members of various long COVID support groups worldwide, including the network Body Politic, from which the PLRC originated. When the authors analysed the data, they found scores of symptoms in at least ten organ systems.
The study showed that the most prevalent problems were fatigue, post-exertional malaise — a worsening of symptoms after exertion — and the cognitive dysfunction that came to be referred to as brain fog. Nearly 86% of participants reported relapses triggered by exertion; 87% said fatigue was a main symptom; and 88% reported brain fog, with no differences in cognitive issues across age groups.
NIH launches trials for long COVID treatments: what scientists think
The paper has amassed more than 1,000 citations, been mentioned in some 60 policy statements and is widely considered a seminal paper in long COVID research, owing to its in-depth analysis. For McCorkell, however, its impact is more fundamental. “What we demonstrated with the survey is that patients can lead high-quality research, and that it’s really necessary in order to have the most comprehensive look at a condition.”
The achievement is especially notable considering that the study was conducted by unpaid volunteers, most of whom identify as disabled, and it received no financial support. By contrast, many long COVID research initiatives have tended to focus on a subset of symptoms, which comes with the risk of missing the bigger picture, says McCorkell.
“There’s a lot of complexity in these illnesses, and I think it’s really important to embrace these complexities,” says Beth Pollack, a research scientist at the Massachusetts Institute of Technology in Cambridge, whose work focuses on understanding long COVID and other infection-associated chronic illnesses. With conditions that have a range of symptoms, and for which there is only limited research, building a knowledge base starts by listening to patients’ stories and capturing the nuances of their conditions, Pollack says.
Desperate measures
In early 2020, Martha Eckey, a pharmacist in Minneapolis, Minnesota, developed a COVID-like illness. She experienced a crushing fatigue that no amount of sleep could relieve, and was bedbound for days at a time. The physicians she went to for help had no answers. In desperation, Eckey turned to the online community of people with long COVID.
She found people trying treatments from prescription medications to over-the-counter supplements. But the effectiveness of these was restricted largely to personal anecdotes.
In the hope of getting a more comprehensive, systematic understanding of what worked, Eckey designed a survey called TREAT ME, which asked people with long COVID and those with myalgic encephalomyelitis, also known as chronic fatigue syndrome (ME/CFS), about their experiences, including whether they had tried any of a list of 150 medications and supplements. More than 4,000 people responded.
Martha Eckey’s TREAT ME survey found overlap between treatments people were using for long COVID and for other chronic conditions.Credit: John Karp
Eckey found overlap with other chronic conditions. Some treatments revealed by the survey as most effective for long COVID were drugs such as beta blockers and the heart-failure medication Corlanor (ivabradine). These are sometimes used to treat postural orthostatic tachycardia syndrome, a nervous-system disorder that can be triggered by COVID-19. Eckey also found that a number of individuals reported relief after taking naltrexone, a non-opioid drug for treating substance-use disorder. When taken at low doses, it has anti-inflammatory and pain-relieving properties.
Physiotherapist David Putrino, who specializes in rehabilitation and human performance at the Icahn School of Medicine at Mount Sinai in New York City, says that the TREAT ME survey captured something both simple and profoundly important. “It’s a very fundamental question of, ‘what are you taking that’s helping right now?’” he says. The results have helped to guide his research on long COVID.
Listening to patients
TREAT ME attracted the attention of scientists and research foundations, who soon realized that this information could help to shape their efforts. One was the Open Medicine Foundation, a non-profit organization in Agoura Hills, California, that studies infection-associated chronic illnesses such as long COVID and ME/CFS.
Linda Tannenbaum, a clinical laboratory scientist, founded the Open Medicine Foundation in 2012 in response to the difficulties she encountered while seeking a diagnosis and treatment for her daughter, who has ME/CFS. Its first double-blind, randomized, placebo-controlled clinical trial will explore low-dose naltrexone (LDN) and another drug, pyridostigmine, which is used to treat an autoimmune disorder that affects voluntary muscle movements. The medications will be tested separately and in combination. Tannenbaum credits TREAT ME for helping to shape which symptoms will be assessed during the trial.
“The reason we are doing LDN as our first trial is that patients asked for it,” she says. TREAT ME also showed that many people with long COVID said that LDN helped to reduce brain fog (see go.nature.com/3qy2tpj). Given these results, the Open Medicine Foundation also incorporated parameters in the trial to test cognitive function. Both LDN and pyridostigmine have been used to treat long COVID, but as many patients report, physicians are often reluctant to prescribe these drugs because of a lack of formal, randomized, controlled trials showing their effectiveness. “Doctors are very hesitant to go outside approved, or at least medically tested, medications,” says Bateman. In her experience, insurance companies also won’t pay for these medications for people with ME/CFS and long COVID without strong evidence to support their use.
Many patient advocates say that there is insufficient clinical research on the kinds of drug that people are already using. In February, the RECOVER initiative received a further $515 million over the next 4 years to test more interventions and investigate the long-term effects of a SARS-CoV-2 infection. But so far, the only trials it has begun are of the antiviral medication Paxlovid (nirmatrelvir and ritonavir), which started enrolling patients in July 2023, and of ivabradine and intravenous immunoglobulin, which recruited its first participants last month.
Lauren Nichols, a long COVID patient advocate, helped to lead the Body Politic support group.Credit: Lauren Owens Lambert/Reuters
“There are a lot of clinical trials that are focused on more behavioural and on non-pharmaceutical interventions, and that is really not a priority to the patient community,” McCorkell says. “It is a misunderstanding of how severe the condition is, and how much of an impact on people’s quality of life it has taken.”
A spokesperson for RECOVER told Nature that the clinical trial of a computer game has already started enrolling participants and that the exercise trial is still scheduled to begin. They emphasized that these are accessible interventions, which might help some people who are affected, given the wide range of symptoms. They also said that moving these trials forwards will help in developing the framework for testing more treatments.
Lifting the fog
In the weeks after her initial COVID-19 infection, Hannah Davis found herself struggling with severe brain fog, to the point at which she could barely string two sentences together. Davis, who at the time was working as a data analyst and artist, with a particular focus on addressing biases in machine learning, kept waiting for her cognitive function to go back to normal, only for it never to return. “I had, and continue to have, terrible, terrible cognitive impairment,” says Davis, who is one of the co-founders of the PLRC.
Long COVID exercise trials proposed by NIH raise alarm
Brain fog is having a significant impact on people’s livelihoods, says Wes Ely, a physician-scientist who works in intensive care at Vanderbilt University Medical Center in Nashville, Tennessee. People with long COVID have a form of cognitive impairment that is often “like mild and moderate dementia”, he says.
Ely, who studies treatments for Alzheimer’s disease and related dementias, decided in 2020 to expand into studying the cognitive impairments associated with long COVID. He quickly recognized that the condition is deeply complex, with symptoms that go beyond cognitive impairment.
To gain a comprehensive understanding of the phenomenon, he turned to the patient community, eventually recruiting Davis and Jaime Seltzer, director of scientific and medical outreach at the non-profit organization ME Action in Santa Monica, California. Together, they drafted a clinical trial to test the medication baricitinib, an immunomodulatory drug that is used to treat rheumatoid arthritis and alopecia areata, and acute COVID-19 infections. “I wanted to learn from people who are living with this disease,” says Ely.
The trio, along with other US investigators, designed a 550-person clinical trial of baricitinib as a potential treatment for long COVID. The trial has now been funded by the NIH and will start enrolment later this year.
From Seltzer’s perspective, an effective collaboration between patients and scientists can help both sides equally, because it leads to more effective and targeted research. “We have the resources to help you do what you do even better,” Seltzer says. The lived experiences of patients can shape research priorities in several key ways, she says. These include finding the most efficient way to allocate limited funds on the basis of symptom burden; offering context on the prevalence and severity of symptoms; and identifying how the trial design can capture improvement most effectively. All of this can help lead to faster breakthroughs in treatments, which is of benefit to both patients and researchers, Seltzer says.
Microclot mystery
In late autumn 2022, McCorkell flew to New York City to participate in a trial being conducted by Putrino and his team. This study aimed to look for the presence of tiny blood clots, called microclots, in people with long COVID. It is thought that these cause symptoms such as fatigue and brain fog by impairing blood flow to the brain and body. There are still a lot of unknowns about microclots, including how many people with long COVID have them, how they form and whether the association is causal.
Long-COVID treatments: why the world is still waiting
McCorkell gave blood samples that were analysed using fluorescent microscopy, which confirmed she had microclots. McCorkell says it was “a wake-up call”. Until that point, she had been managing her symptoms mainly by avoiding overexertion. But the presence of the clots suggested to her that there might be active damage happening to her body. So, she started taking supplements that TREAT ME survey respondents reported as helpful.
Eckey’s results, which have not yet been published in a peer-reviewed journal, show that of 668 respondents with long COVID, between 40% and 70% found some symptom relief when taking the supplements nattokinase, serrapeptase or lumbrokinase, individually or in combination (see go.nature.com/43xgyoq).
When Putrino saw these results, he decided it was crucial to conduct clinical trials of the supplements. He expects to begin a 120-person study on lumbrokinase in the coming months, and has involved patients at every step of its development.
“Every research trial that we run, we involve the patient community in the protocol,” Putrino says. This includes taking their advice on what trials should be prioritized, what symptoms to assess, how many clinic visits to require and what the testing environment should be like, to minimize the risk of exacerbating their symptoms, he says.
McCorkell says that the supplements she’s been taking have improved her general function by about 10%. Whereas that might not sound like much, she feels it is meaningful progress. Although the long COVID research has been difficult, she sees no other option but to stay involved. “We’re driven by desperation, out of improving our own quality of life.”
In February, I was meant to speak at the European Conference of Tropical Ecology in Lisbon, providing evidence of extinction risks to some frog species used as bushmeat in West Africa, and highlighting the need for policies that regulate hunting pressures.
In January, I duly applied at the Dutch embassy in Accra for a business visa to the European Union Schengen area. My application included the invitation from the conference organizers, a letter from my sponsors — the Center for International Forestry Research and World Agroforestry, and the UK Global Challenges Research Fund’s Trade, Development and the Environment Hub — and an introductory letter from the dean of graduate studies at the University of Ghana, confirming my status as a final-year PhD candidate. It also included current and old passports that showed my extensive travels, mostly to the United Kingdom.
Tear down visa barriers that block scholarship
Almost three weeks later, my passport was returned with a rejection note, stating that I had not provided justification for the purpose and conditions of my intended stay, and that there were reasonable doubts about my intention to leave the EU before the visa expired.
I wasn’t the only one. Of the ten speakers from low- and middle-income countries (LMICs) invited to present at the conference’s “Wildmeat: opportunities and risks” session, only four got visas. Another person withdrew voluntarily.
The participation of researchers from LMICs at international conferences on biodiversity is of the utmost importance. Earth’s biodiversity is richest in these nations, and includes ecosystems that provide important services, such as carbon sequestration, that benefit people globally. Our participation is not a matter of simply ticking the inclusivity boxes, but a deliberate effort to ensure that the voices of people for whom some of these conservation policies are formulated are heard, and their opinions sought.
However, whereas colleagues from wealthy nations, even as undergraduate students, can easily go to LMICs to participate in conferences and do research, the same cannot be said for those going the other way. The same documentation that scientists from high-income countries present at embassies — sponsorship, invitation and introductory letters — are apparently inadequate when submitted by people from LMICs. According to a global survey in 2018 by the research organization RAND, African and Asian researchers are the most likely to have visa-related challenges for short-term visits (see go.nature.com/2z9dabp). A 2023 analysis by the Royal Society in London showed that in 2022, of the 30 territories for which the United Kingdom refused visitor visas most often, 22 were in Africa (see go.nature.com/3vxruba).
Battles over funding could threaten historic effort to save species
These refusals come at a huge cost to individual researchers. Visa applications require scientists to be studious with paperwork, commit often large sums of money and make several trips to embassies that are sometimes outside their home country. My experience left me feeling demoralized, embarrassed and insulted by the implication that I and people like me couldn’t be trusted to attend a conference without outstaying our welcome.
This broken situation also comes at a cost to institutions. My sponsor spent approximately US$1,500 on my visa fee, return flight, insurance and conference registration (all non-refundable). Conference organizers and host institutions in wealthy countries spend a lot of time and effort searching for and inviting credible and accomplished researchers from LMICs to be part of the global conservation effort — time and money that is often wasted, which then discourages meeting organizers from prioritizing speakers from those nations.
Moreover, it comes at a cost to global efforts to prevent further biodiversity loss. Many high-income countries say that they are committed to global biodiversity conservation, and governments are pledging billions of dollars in support. Their visa policies for researchers should reflect this priority.
It’s time for countries to honour their million-dollar biodiversity pledges
I am not suggesting that embassies should operate without caution and issue visas without due diligence. But they should ensure that eligible candidates who meet the criteria are not prevented from participating in international discourse. This requires a distinct form of short-term visa review for scientists attending conferences, seminars, workshops and research programmes, and a commitment to improve communication channels between visa-issuing authorities, conference organizers and academic institutions, both in the countries hosting the events and in those that researchers are travelling from.
Part of this is ensuring that entry-clearance officers do not fixate on a scientist’s financial worth as a measure of the credibility of their intent to return to their home countries. Bank statements are often required to support visa applications. Mine show the grants I have received from the Rufford Foundation, Synchronicity Earth and the BaNGA-Africa/Carnegie Corporation of New York. Others are not so fortunate, and this approach risks allowing only well-off, established scientists to obtain short-stay visas — automatically preventing many early-career researchers from participating in global research conversations.
Conferences are where research collaborations are formed and where decisions on funding, publishing and policymaking are made. It is imperative that visa issues do not block scientists from LMICs benefiting from the opportunities they provide.
Generative AI might be a powerful tool in making research more accessible for scientists and the broader public alike.Credit: Getty
Thinking back to the early days of her PhD programme, Esther Osarfo-Mensah recalls struggling to keep up with the literature. “Sometimes, the wording or the way the information is presented actually makes it quite a task to get through a paper,” says the biophysicist at University College London. Lay summaries could be a time-saving solution. Short synopses of research articles written in plain language could help readers to decide which papers to focus on -— but they aren’t common in scientific publishing. Now, the buzz around artificial intelligence (AI) has pushed software engineers to develop platforms that can mass produce these synopses.
Scientists are drawn to AI tools because they excel at crafting text in accessible language, and they might even produce clearer lay summaries than those written by people. A study1 released last year looked at lay summaries published in one journal and found that those created by people were less readable than were the original abstracts -— potentially because some researchers struggle to replace jargon with plain language or to decide which facts to include when condensing the information into a few lines.
AI lay-summary platforms come in a variety of forms (see ‘AI lay-summary tools’). Some allow researchers to import a paper and generate a summary; others are built into web servers, such as the bioRxiv preprint database.
AI lay-summary tools
Several AI resources have been developed to help readers glean information about research articles quickly. They offer different perks. Here are a few examples and how they work:
– SciSummary: This tool parses the sections of a paper to extract the key points and then runs those through the general-purpose large language model GPT-3.5 to transform them into a short summary written in plain language. Max Heckel, the tool’s founder, says it incorporates multimedia into the summary, too: “If it determines that a particular section of the summary is relevant to a figure or table, it will actually show that table or figure in line.”
– Scholarcy: This technology takes a different approach. Its founder, Phil Gooch, based in London, says the tool was trained on 25,000 papers to identify sentences containing verb phrases such as “has been shown to” that often carry key information about the study. It then uses a mixture of custom and open-source large language models to paraphrase those sentences in plain text. “You can actually create ten different types of summaries,” he adds, including one that lays out how the paper is related to previous publications.
– SciSpace: This tool was trained on a repository of more than 280 million data sets, including papers that people had manually annotated, to extract key information from articles. It uses a mixture of proprietary fine-tuned models and GPT-3.5 to craft the summary, says the company’s chief executive, Saikiran Chandha, based in San Francisco, California. “A user can ask questions on top of these summaries to further dig into the paper,” he notes, adding that the company plans to develop audio summaries that people can tune into on the go.
Benefits and drawbacks
Mass-produced lay summaries could yield a trove of benefits. Beyond helping scientists to speed-read the literature, the synopses can be disseminated to people with different levels of expertise, including members of the public. Osarfo-Mensah adds that AI summaries might also aid people who struggle with English. “Some people hide behind jargon because they don’t necessarily feel comfortable trying to explain it,” she says, but AI could help them to rework technical phrases. Max Heckel is the founder of SciSummary, a company in Columbus, Ohio, that offers a tool that allows users to import a paper to be summarized. The tool can also translate summaries into other languages, and is gaining popularity in Indonesia and Turkey, he says, arguing that it could topple language barriers and make science more accessible.
Despite these strides, some scientists feel that improvements are needed before we can rely on AI to describe studies accurately.
Will Ratcliff, an evolutionary biologist at the Georgia Institute of Technology in Atlanta, argues that no tool can produce better text than can professional writers. Although researchers have different writing abilities, he invariably prefers reading scientific material produced by study authors over those generated by AI. “I like to see what the authors wrote. They put craft into it, and I find their abstract to be more informative,” he says.
Is ChatGPT making scientists hyper-productive? The highs and lows of using AI
Nana Mensah, a PhD student in computational biology at the Francis Crick Institute in London, adds that, unlike AI, people tend to craft a narrative when writing lay summaries, helping readers to understand the motivations behind each step of the study. He says, however, that one advantage of AI platforms is that they can write summaries at different reading levels, potentially broadening the audience. In his experience, however, these synopses might still include jargon that can confuse readers without specialist knowledge.
AI tools might even struggle to turn technical language into lay versions at all. Osarfo-Mensah works in biophysics, a field with many intricate parameters and equations. She found that an AI summary of one of her research articles excluded information from a whole section. If researchers were looking for a paper with those details and consulted the AI summary, they might abandon her paper and look for other work.
Andy Shepherd, scientific director at global technology company Envision Pharma Group in Horsham, UK, has in his spare time compared the performances of several AI tools to see how often they introduce blunders. He used eight text generators, including general ones and some that had been optimized to produce lay summaries. He then asked people with different backgrounds, such as health-care professionals and the public, to assess how clear, readable and useful lay summaries were for two papers.
“All of the platforms produced something that was coherent and read like a reasonable study, but a few of them introduced errors, and two of them actively reversed the conclusion of the paper,” he says. It’s easy for AI tools to make this mistake by, for instance, omitting the word ‘not’ in a sentence, he explains. Ratcliff cautions that AI summaries should be viewed as a tool’s “best guess” of what a paper is about, stressing that it can’t check facts.
Broader readership
The risk of AI summaries introducing errors is one concern among many. Another is that one benefit of such summaries — that they can help to share research more widely among the public — could also have drawbacks. The AI summaries posted alongside bioRxiv preprints, research articles that have yet to undergo peer review, are tailored to different levels of reader expertise, including that of the public. Osarfo-Mensah supports the effort to widen the reach of these works. “The public should feel more involved in science and feel like they have a stake in it, because at the end of the day, science isn’t done in a vacuum,” she says.
But others point out that this comes with the risk of making unreviewed and inaccurate research more accessible. Mensah says that academics “will be able to treat the article with the sort of caution that’s required”, but he isn’t sure that members of the public will always understand when a summary refers to unreviewed work. Lay summaries of preprints should come with a “hazard warning” informing the reader upfront that the material has yet to be reviewed, says Shepherd.
Why scientists trust AI too much — and what to do about it
“We agree entirely that preprints must be understood as not peer-reviewed when posted,” says John Inglis, co-founder of bioRxiv, who is based at Cold Spring Harbor Laboratory in New York. He notes that such a disclaimer can be found on the homepage of each preprint, and if a member of the public navigates to a preprint through a web search, they are first directed to the homepage displaying this disclaimer before they can access the summary. But the warning labels are not integrated into the summaries, so there is a risk that these could be shared on social media without the disclaimer. Inglis says bioRxiv is working with its partner ScienceCast, whose technology produces the synopses, on adding a note to each summary to negate this risk.
As is the case for many other nascent generative-AI technologies, humans are still working out the messaging that might be needed to ensure users are given adequate context. But if AI lay-summary tools can successfully mitigate these and other challenges, they might become a staple of scientific publishing.
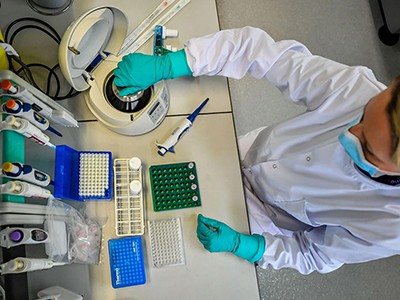
One in four Black men will be diagnosed with prostate cancer.Credit: Getty
Olugbenga Samuel Oyeniyi’s research at the University of Sunderland, UK, explores why many Black men do not seek help for symptoms of prostate cancer and uses Black peer educators to change mindsets in the community. March is Prostate Cancer Awareness Month in the United Kingdom.
What drew you to research?
I worked in a hospital laboratory in Enugu in southeastern Nigeria after completing a bachelor’s degree in microbiology at Obafemi Awolowo University in Ile-Ife in 2006. Then I did a one-year master’s programme in biomedicine at the University of Portsmouth, UK, researching glioblastoma. My heart was set on academia, so in 2014, after working as a pre-clinical-trials research scientist based in industry, I started a PhD in applied microbiology at the University of Sunderland, looking at the Acanthamoeba parasite, which can cause blindness, among other things.
How did you get into prostate-cancer research?
In December 2020, I got a job as a senior scientist overseeing COVID-19 samples in a lab in Gateshead, UK, eventually becoming operations manager, which involved working with the University of Sunderland’s vice-chancellor, the local mayor and a member of Parliament. After the lab closed in May 2022, I saw an advert for a postdoctoral research associate in public health with a focus on prostate cancer. I automatically thought it was not for me — I was a clinical scientist dreaming of finding a cure for malaria. But then I read that one in four Black men will be diagnosed with prostate cancer, compared with one in eight white men, according to UK figures. That got my attention. I had a further look and it said one in 12 of those will die of it, compared with one in 24 white men. I thought, “Woah, this is affecting me” — I’m the eldest of four brothers. And not just me, but my community.
Nature Outlook: Prostate cancer
I started in September 2022, coordinating the research for Early Diagnosis of Prostate cancer for Black Men (PROCAN-B) project. It’s funded by Prostate Cancer Research, a London-based charity that supports research in this field in the United Kingdom and the United States.
Our aim is to reduce the obstacles to early diagnoses and save lives. What makes this work special is that it is research for Black men in the community, facilitated by Black men in the community, coordinated by a Black researcher.
How does the project work?
Our team includes public-health researchers, behavioural scientists, a psychologist, myself as project manager and two research assistants from the Black community who recruit the focus-group participants.
In October 2022, we created a community-led advisory and engagement group (also known as public involvement and community engagement, or PICE) made up of 13 Black men aged 47–63 from two parts of the United Kingdom: the northeast of England and Scotland. None of them had experienced prostate cancer personally, but one had a brother who was being treated for the disease.
We met three times to discuss the barriers to diagnosis and had a further three meetings to co-design interventions, such as community workshops to tackle some of these barriers to diagnosis. Then we had a further three meetings to train the group as peer facilitators to deliver the workshops. The first workshops took place in Sunderland and Glasgow in November 2023, with ten participants in each. We had feedback sessions a month later and used this information to refine the community workshops. We found that the men were interested and engaged in the pilot sessions — there were questions about every presentation slide.
Olugbenga Samuel Oyeniyi’s interests now lie in public health and epidemiology.Credit: University of Sunderland
So, we gave the men a piece of paper to write down their questions and we moved the Q&A part of the session with a general medical practitioner (GP), who was from the Black community, from the middle of the session to the end.
We held further workshops with 20 men each in Middlesborough and Glasgow in February. In Middlesborough, the men were so engaged. We were supposed to finish at 8 p.m., but there were still so many questions for the GP that we went on for another hour.
Why do Black men with symptoms sometimes avoid getting help?
Trust is a big issue: lack of trust in the statistics; in the health-care system; and in GPs. Men might have had negative experiences with gatekeepers such as the GP surgery receptionist, for example. There are also religious and cultural factors, such as social stigma.
The PICE group noted that talking about intimate and sensitive health issues such as prostate cancer is difficult for Black men because it can be embarrassing. Discussing intimate issues was a challenge related to sexuality and manhood. Group members also believed that Black men are raised to feel ‘super’, or stronger than women, which makes it difficult to show weakness and vulnerability.
You also identified structural racism as a barrier. Can you tell us about that?
Some of the participants described experiencing discrimination and racism in the health-care system. They feel they are treated differently and the same standards of care aren’t applied or don’t apply to Black people. One participant commented that health-care providers’ questions regarding medical conditions visible through changes to skin colour are written for white people and might not be applicable to a Black man. In another example, most of the statistics posted in bus-stop and train-station campaign ads say prostate cancer affects one in eight men. This is also part of structural racism — those are the figures for white men.
Your campaign involved video footage of British actor Idris Elba and US actor Morgan Freeman. Tell us how that helped.
These men are incredibly influential and in 2021 filmed Embarrassed, a powerful video from Black UK film director Steve McQueen, which was part of a separate campaign. We use it to inform the focus groups.
We also use videos of UK religious leaders — a pastor and an imam — and Black male survivors of prostate cancer. Other videos involve women, some of whom appeal to the men’s emotional side, saying “Your health is important to us and your families — look after your prostate health.”
How does PROCAN-B fit alongside other Prostate Cancer Research funding?
Our research is one of several projects the charity has funded as part of its racial-disparity funding call, particularly focused on Black men and prostate cancer. For example, one study from the University of Essex in Colchester, UK, has found that genetic mutations could help to explain why Black men are at higher risk of developing prostate cancer than are men of other ethnicities.
What is the future for the research — and for you?
If the workshops continue to be successful and our research shows they are making an impact, they could be rolled out across the country with a much larger group of people in a randomized controlled trial, depending on funding.
My current contract is due to end in August 2024. I want to continue with research, become a senior lecturer and do a master’s in public health, ideally at one of the top UK universities, potentially the University of Edinburgh or the London School of Hygiene & Tropical Medicine.
I believe the combination of laboratory studies and public-health research is key and crucial to comprehensive and extensive understanding of human health.
Eventually, my goal is to become a professor of public health and epidemiology, and to collaborate with researchers back home to address some of the health challenges facing Nigeria.
Last year, the Nature Index was broadened to include author affiliations from articles in more than 60 medical journals. The expansion, which covers all major disciplines and specialities in clinical medicine and surgery, offers new insights into global publishing trends in the health sciences. This is the first supplement to explore some of those trends.
The second noticeable data point is the dominance of Harvard University in the field. The institution, based in Cambridge, Massachusetts, has a Share (822) that is almost three times higher than the second-ranked institution, the US National Institutes of Health (290).
An extraordinary amount of money is invested in health-sciences research, but this hasn’t translated to a faster pipeline for new therapies. The increasing complexity of clinical trials is part of the problem, and something that researchers are hoping artificial intelligence can help to address. Others are rethinking how therapies are assessed in trials to make the results more meaningful. For example, could data impact people with Alzheimer’s and other progressive conditions by measuring how many ‘good years’ a medication can give, rather than comparing scores on cognitive tests?
Outside clinical trials, there are structural weaknesses in health-sciences research that need urgent attention, such as the lack of women in leadership positions. If institutions do not work harder to increase diversity at the top levels of academia, they risk damaging the talent pipeline and ultimately health outcomes for everyone.
As the leading country in health-sciences output in the Nature Index, the United States’ Share is almost 8,500, higher than the next 10 leading countries combined. As a result, US institutions feature prominently among the leading research organizations for the subject, with 30 of the top 50 being based there.
The country’s dominance means that it comes top for Share in all but seven of the journals tracked by the Nature Index in the subject. This includes large general journals such as Nature Communications and specialist medical publications such as The New England Journal of Medicine. PLOS Medicine and Gut are two examples where authors based elsewhere (the United Kingdom and China) made the largest contribution.
Source: Nature Index. Data analysis by Aayush Kagathra. Infographic by Simon Baker, Bec Crew and Tanner Maxwell.
The United States is the clear frontrunner among the leading five countries for health-sciences research, with a Share almost four times higher than China, in second place. The United Kingdom is third, with a Share of almost 1,500, a higher placing than its fourth position overall in the Nature Index.
Source: Nature Index. Data analysis by Aayush Kagathra. Infographic by Simon Baker, Bec Crew and Tanner Maxwell.
Out of the top 25 countries for health-sciences articles in the Nature Index, five nations have a Share that makes up at least 29% of their overall footprint in the database across all subjects. Denmark, whose research is boosted by the success of companies such as Novo Nordisk, has the highest ratio in this regard at almost 40%.
Source: Nature Index. Data analysis by Aayush Kagathra. Infographic by Simon Baker, Bec Crew and Tanner Maxwell.
As Harvard University, in Cambridge, Massachusetts, is the leading institution for high-quality health-sciences research, its involvement in the top institutional partnership in the field is no surprise. But its dominance does not extend to all the other leading collaborations, some of which involve institutions outside the United States.
Source: Nature Index. Data analysis by Aayush Kagathra. Infographic by Simon Baker, Bec Crew and Tanner Maxwell.
The difference in Nature Index health-sciences output between the leading academic institution, Harvard University in Cambridge, Massachusetts, and other top institutions is a Share of more than 600. Compared with Harvard, most of the leading institutions also have a lower proportion of their overall Nature Index output in health sciences.
The University of Toronto in Canada and Johns Hopkins University in Baltimore, Maryland, are the only other academic institutions with a health-sciences Share of over 200. They also have a relatively strong focus on health sciences, with over 35% of their overall Nature Index research output in the subject area.
Source: Nature Index. Data analysis by Aayush Kagathra. Infographic by Simon Baker, Bec Crew and Tanner Maxwell.
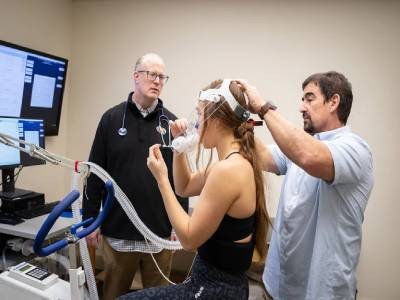
Siri Eldevik Håberg studies whether environmental factors such as smoking are linked to subtle changes to the human genome.Credit: Fredrik Naumann/Panos Pictures for Nature
As a medical student, Siri Eldevik Håberg became fascinated with how the health of a baby can be affected during pregnancy. Smoking, for example, is a proven risk factor for respiratory infection in fetuses — a finding supported by one of Håberg’s earliest studies, which scoured data from tens of thousands of births in Norway to investigate outcomes for a small subset of women who had smoked during, but not after, pregnancy1. The analysis was based on data from the Mother, Father, and Child Cohort Study (MoBa) at the Norwegian Institute of Public Health (NIPH) in Oslo, which today holds biological samples and survey information for nearly 300,000 participants.
Nature Index 2024 Health sciences
Håberg conducted her postdoctoral work in the United States, where she joined a group at the National Institute of Environmental Health Sciences in Durham, North Carolina. She contributed data analysis to a team that examined 1,062 blood samples from MoBa, drawn from the umbilical cord at the delivery of a baby, and identified 10 genes that were altered in infants born to women who smoked while pregnant. The 2012 study provided important evidence for how non-heritable smoking exposure can cause certain epigenetic effects — subtle changes to the genome that impact the reading of DNA but do not alter the DNA sequence2. “We are only beginning to understand the gravity of epigenetic changes during development,” says Håberg.
Now, as director of the Centre for Fertility and Health at the NIPH, Håberg is investigating ways to combine MoBa data with statistics from Norwegian registries on factors such as vaccinations, prescriptions, education and economic status. In one project, she and her colleagues matched babies from the 2012 study with data collected by the Medical Birth Registry of Norway and found that reduced birth weight was strongly correlated with smoking during pregnancy3.
Having investigated the effects of smoking on fetal health, Håberg was interested in other factors that could cause epigenetic changes linked to development. In a 2022 study published by Nature Communications4, she and her co-authors compared rates of DNA methylation — a process that affects levels of gene expression — for almost 2,000 MoBa newborns. Roughly half of the babies were conceived naturally and half through reproductive technologies such as in vitro fertilization. Even after controlling for the parents’ DNA methylation rates, differences were found in more than 100 genes, including those related to growth and development. The findings might pave the way for big-data approaches to studies related to reproductive technologies.
Håberg is passionate about connecting specialists from her team with interdisciplinary groups from around the world so that they can explore large amounts of data that hold clues about fetal health. One such project is comparing MoBa data with information from the Danish National Birth Cohort. “It all comes down to finding exciting new ways for teams of specialists to work together,” she says. “It’s great to see so many resources dedicated to questions of early embryonic development.” — Amy Coombs
NARMIN GHAFFARI LALEH: Deeper vision
Narmin Ghaffari Laleh.Credit: Courtesy of Narmin Ghaffari Laleh
As a university student studying medical photonics in Jena, Germany, Narmin Ghaffari Laleh was inspired to use her programming skills to help patients and doctors. She sought work experience at local medical-device company, Carl Zeiss Meditec, to explore the use of artificial intelligence (AI) in improving medical-image analysis. Her work there concentrated on eye imaging, where conventional methods of analysis use systems that read each row of pixels, identifying features such as the cornea, lens and retina by tracking their colours and the distance between them. Common variables such as glasses can throw such systems off, however. “These kinds of programs work well until someone puts on glasses or contact lenses and takes a photo,” says Ghaffari Laleh, who was a master’s student at Fredrich Schiller University of Jena at the time.
The model developed by Ghaffari Laleh and her colleagues at the company used deep learning — a machine-learning technique that can identify complex patterns. In testing, their system analysed images with variables such as glasses with greater accuracy and less human oversight than previous methods. “I saw the potential for this sort of program to impact other areas of medicine, because the machine-learning techniques were rapidly becoming more sophisticated and could handle more data, all without the traditional human reviewer,” says Ghaffari Laleh, who built on these findings in her 2020 master’s thesis.
Ghaffari Laleh began her PhD at RWTH Aachen University in Aachen, Germany, in the field of computational pathology — an emerging area of research that aims to improve patient care by using advances in AI and big data. Her focus was on developing systems that can more accurately and efficiently identify visual indicators of cancer and other diseases than methods that rely solely on human specialists. These systems could be particularly useful in the analysis of tissue samples that have been prepared for microscope slides and stained with the widely used haematoxylin and eosin (H&E) dye, which turns cell structures different shades of purple, blue and pink, she says.
In 2022, Ghaffari Laleh co-authored a paper5 describing how AI could consistently categorize tumours in kidney-tissue slides. “With deep learning, we can detect patterns that the human eye cannot see,” she says.
For a separate study6, the team showed how AI trained to identify mutations in a protein associated with bladder cancer could outperform a uropathologist in analysing tissue samples stained with H&E. “We do not aim to replace the urologist, but deep-learning can offer additional analysis,” says Ghaffari Laleh.
To test whether these methods can move to clinical applications, Ghaffari Laleh dedicated her PhD thesis to investigating how applicable these kinds of AI systems could be to a variety of diseases and patient demographics. Her dissertation is pending defence in March.
Ghaffari Laleh hopes to apply her skills to help medical professionals in developing countries who cannot afford to run advanced diagnostics and who struggle to recruit and train skilled professionals. “AI is a much more affordable option,” she says. “If a deep-learning model can analyse data from diverse patient groups from a wide range of countries, then hospitals that lack resources can ship samples for diagnosis.” She’s also working on AI that can read text7, ultrasound and radiology image data, with hopes that they can speed up the work of doctors and other specialists worldwide. — Amy Coombs
TAL PATALON: Prolific polymath
Tal Patalon.Credit: Asaf Brenner
Tal Patalon prides herself on being able to pivot her work to where she thinks her expertise, and that of her team, will be most effective. “For me, it’s all about clinical impact,” she says. As head of Kahn-Sagol-Maccabi (KSM) in Tel Aviv — the research and innovation centre of Maccabi Healthcare Services, one of Israel’s largest health-care providers — Patalon is interested in a range of medical conditions, including parvovirus, mpox, cancer and coeliac disease.
Having the capacity to launch research projects quickly proved invaluable to Patalon and her team during the COVID-19 pandemic, when global treatment and vaccination protocols changed rapidly to keep up with the evolution of the disease. In 2021, as the highly contagious Delta wave was surging through Israel, Patalon co-led a team that scoured the health records of almost 125,000 Israelis, charting coronavirus incidence, symptoms and hospitalization rates over three months.
The team discovered that vaccinated people who had not previously tested positive for COVID-19 were 13 times more likely to be infected by the new variant, compared with previously infected individuals who were unvaccinated. The results showed that the SARS-CoV-2 virus that causes COVID-19 confers a natural immunity to those who have been infected, providing valuable evidence that vaccinating them wasn’t an immediate priority8. “It was a very big achievement for us,” says Patalon.
Extracting new insights from the vast amounts of public-health data that are being collected globally is key to advancing treatments and keeping one step ahead of infectious diseases, says Patalon. As part of her role at KSM, she oversees the Tipa Biobank, Israel’s largest biosample repository, comprising more than one million blood samples from some 200,000 Maccabi patients. In addition to one-off samples from patients, the biobank collects serial samples — successive samples from the same patient over a period of time. Serial samples are “very rare and highly valuable for research”, says Patalon, especially when it comes to analysing biological changes before and after a diagnosis.
KSM also manages some 30 years’ worth of electronic medical records from more than 2.7 million patients collected by 32 hospital networks that are affiliated with Maccabi. By sharing these data, which have been deidentified, with researchers around the world, Patalon hopes to inform artificial-intelligence-powered innovations in diagnosis and treatment. “These collaborations, I believe, will create the future of medicine,” she says.
Being adaptable as a researcher and a leader is crucial, particularly in times of crisis, says Patalon, whose team has been deeply affected by the war in Gaza.
“This is a time that requires a lot of patience, empathy, emotional support and the building of good relationships. We have to come out of this situation stronger.” — Sandy Ong
SARAH LUO: Hunting hunger pathways
Sarah Lou’s team discovered one of the brain’s many feeding regulatory centres.Credit: Agency for Science, Technology and Research (A*STAR)
Sarah Luo’s fascination with neuroscience sparked when, as an undergraduate student at the University of Wisconsin-Madison in Wisconsin, she was introduced to the work of British neurologist and author, Oliver Sacks.
Known for his empathic approach to patients with conditions such as amnesia, face blindness and Tourette’s syndrome, Sacks “brought a very humanizing perspective to brain disorders”, says Luo. “He showed how even minute changes in certain regions of the brain could lead to profound effects on cognition and behaviour.”
Today, Luo runs a lab at Singapore’s Agency for Science, Technology and Research (A*STAR), where she studies the connection between hunger and the brain to help patients with metabolic disorders such as diabetes and fatty liver disease. She first studied this connection as a postdoctoral fellow in an adjacent lab, where she was part of a team that discovered a mechanism that regulates feeding.
For many years, researchers had assumed that hunger is regulated by two types of neurons: one that drives hunger and another that suppresses it. But when Luo and her colleagues ran experiments that stimulated certain neurons in a region of the brain called the tuberal nucleus, they could prompt mice to start eating even when they weren’t hungry9. “There are actually many feeding regulatory centres in the brain, and we discovered one of them,” she says.
These other centres can deal with “more diverse aspects of eating behaviour”, says Luo, including environmental cues that can incite hunger. In a series of follow-up experiments10, Luo and her colleagues observed that when mice were placed in the same feeding chamber where the neurons in the tuberal nucleus had been activated the previous week, they would immediately start eating, even if it was outside their normal feeding times. The results suggest that these neurons not only influence basic feeding behaviour, but also integrate memory and contextual cues into the eating process, says Luo.
Humans experience similar cues. Visiting a favourite restaurant, for example, or returning to the family home can spark an appetite.
“Your neurons might become activated, just because of the environment you’re in,” says Luo. “Those signals might cause you to eat, even if you’re not actually hungry.”
Luo and her team at A*STAR hope to develop treatments that will help to curb excessive food consumption in people with obesity and metabolic conditions by blocking or activating certain neural signals. The trick, she says, is to find and target pathways that run between the brain and organs such as the liver and kidneys, which are more accessible than neural pathways in the brain.
“It would be very invasive to implant an electrode in the brain to activate or inhibit these pathways,” says Luo. But activating pathways that connect to these regions in the brain — by using vagal nerve stimulation, for example, which is a technique used to treat epilepsy that involves implanting a pulse generator under the skin on the chest — would be a more viable option. “Then maybe there will be an easier route for developing therapies to target some of these metabolic diseases,” says Luo. — Sandy Ong