Hello Nature readers, would you like to get this Briefing in your inbox free every day? Sign up here.
A typical mouse embryo (left) has four limbs. An embryo in which a particular gene was switched off halfway through development has six limbs, and several of its internal organs protrude from its abdomen.Credit: Anastasiia Lozovska et al/Nat. Comms
Developmental biologist Moisés Mallo and his colleagues inactivated a gene in a mouse embryo to see how the change affected spinal-cord development. One of the bioengineered embryos developed genitals that looked similar to two extra hind limbs. The finding led the researchers to unexpected discoveries about which changes in DNA’s 3D structure affect how embryos develop. “I didn’t choose the project, the project chose me,” Mallo says.
South Korea will become the first East Asian country to join the European Union’s €95-billion (US$102-billion) Horizon Europe research-funding programme. The country’s researchers will be eligible to apply for grants from a €53.5 billion pot of funding for research into global challenges in health, energy, climate change and industrial competitiveness. Last year, New Zealand became the first country to ‘associate to’ Horizon Europe, Canada will be signing on later this year, and Singapore and Japan are in preliminary discussions with the European Commission.
Studies in mice reveal that when long-term memories are formed, the DNA in some nerve cells snaps, triggering an immune response responsible for repair. This DNA damage-and-repair cycle might be a way for nerve cells to make memories that last. When mice were trained to remember an electrical shock, the nerve cells initiated an inflammatory response mediated by the TLR9 protein. When the researchers deleted the gene encoding the TLR9 protein from mice, the animals had trouble recalling long-term memories: they forgot the place where they had previously been shocked. These findings contribute to the picture that forming memories is a “risky business”, says neurobiologist Li-Huei Tsai.
Before the collapse of cryptocurrency exchange FTX and the jailing of its chief exec Sam Bankman-Fried, the company allocated tens of millions of dollars to effective altruism — a philanthropic movement dedicated to tackling long-term risks to humanity, such as climate change. This included giving money to research organizations and scientists, many of whom are under pressure to return the money. Some people are concerned that news of the fraud has damaged the perception of effective altruism itself. “We were really gearing up to this big change,” says Sawyer Bernath of the Berkeley Existential Risk Initiative. “All of a sudden it turned out to be all fake.”
Efforts such as the Patient-Led Research Collaborative have played a crucial role in advising, designing and even funding basic and clinical research into long COVID. Its influential survey has amassed more than 1,000 citations. Co-founder Lisa McCorkell is among the patient advocates who say that despite the fact that such efforts can worsen their symptoms, they have little choice but to get involved. “We’re driven by desperation, out of improving our own quality of life.”
A spreadsheet that has been shared between graduate students around the world for more than a decade helps academics in management navigate the job market. Refreshed each year, the spreadsheet’s tabs act as a job-listings board — and a forum for questions and frustrations. “If that sounds similar to Slack and other messaging tools, it is,” writes business researcher Silvia Sanasi. “But the spreadsheet is completely anonymous. It is also incredibly flexible, quick to load and easy to search. Plus, researchers are already well versed in spreadsheets — and appreciate the ability to trawl job-search boards while looking as if they’re working.”
Palaeobotanist Estella Bergere Leopold’s investigations of fossil pollen and spores provided some of the first insights into the evolution of modern plant communities. In 1955, Leopold became one of the few female scientists at the US Geological Survey, where her studies revealed the existence of a tropical rainforest in the south Pacific millions of years ago. Leopold was also an ardent conservationist and activist who traced back her unbridled enthusiasm for ecology to her childhood spent on a farm in Wisconsin. “Without loving nature,” she said in 2011, “who’s going to want to protect it?” Leopold has died, aged 97.
A bird-like brain might have been the ancestral crucible for dreams, writes cultural curator Maria Popova. In ostriches, which belong to the most ancient group of birds, and platypuses, which are part of the most ancient mammal group, dream-like activity was found in the brainstem. In other birds and mammals, dream-rich sleep takes place primarily in the forebrain, suggesting that dreaming slowly migrated into this evolutionarily younger structure. “The most haunting intimation of the research on avian sleep is that without the dreams of birds, we too might be dreamless,” Popova says.
Credit: CTIO/NOIRLab/DOE/NSF/AURA; Image processing: T. A. Rector, Univ. Alaska Anchorage/NSF’s NOIRLab; M. Zamani & D. de Martin, NSF’s NOIRLab
This stunning photo shows the Vela supernova remnant, an expanding nebula of cosmic debris created by a massive stellar explosion around 11,000 years ago. The image was created by separately capturing light of distinct wavelengths using filters and then combining them.
When Lisa McCorkell got COVID-19 in March 2020, her symptoms were mild. Her physicians told her to isolate from others and that she would recover in a few weeks. But the weeks stretched into months and McCorkell, who was working on a master’s degree in public policy at the University of California, Berkeley, started having debilitating and bewildering symptoms: fatigue, dizziness and shortness of breath. Previously an avid runner, McCorkell found her heart racing from simple efforts.
She struggled to find an explanation, and soon realized that her physicians didn’t know any more about her condition than she did. To complicate matters, the limited availability of high-quality testing for the coronavirus SARS-CoV-2 in the early days of the pandemic left many of her doctors wondering whether her symptoms were really due to COVID-19 at all. “I didn’t have health-care providers that took me seriously,” McCorkell says. “That largely pushed me out of the health-care system.”
McCorkell turned instead to those who were experiencing the same puzzling symptoms and frustrations, joining a support group for people with what would eventually be called long COVID. As they compared notes, McCorkell and a handful of others — many of whom had research experience — realized that the information they were sharing might be helpful not only for those with long COVID, but also for those looking to study the condition. So, they founded a non-profit organization, called the Patient-Led Research Collaborative (PLRC), to design, provide advice on and even fund basic and clinical research into long COVID and other chronic illnesses.
Four years on: the career costs for scientists battling long COVID
A survey run by the group and published in 2021 catalogued the more than 200 symptoms experienced by people with the condition (H. E. Davis et al. eClinicalMedicine38, 101019; 2021). It is seen by some as putting long COVID on the map. “They really jump-started the interest,” says Lucinda Bateman, a physician in Salt Lake City, Utah, who specializes in treating people who have long COVID and related conditions. “That was really a point from where more broad awareness arose.”
In the past few years, this study and similar patient-led efforts have helped to shape research programmes on long COVID and kick off some early clinical trials of therapies that might otherwise have gone unexplored. Many patient advocates see the efforts as crucial. They also think the results are more helpful for advancing the understanding of long COVID than the current findings from programmes funded by the US$1.15-billion RECOVER initiative led by the US National Institutes of Health (NIH). People with long COVID and their advocates have criticized the initiative for not always listening to the needs of people with long COVID.
Getting involved in research is challenging, given the symptoms of long COVID, but many patient advocates say they have no choice. “They’ve got you over a barrel,” says Margaret O’Hara, who coordinates patient involvement in research for a National Health Service hospital trust in England. O’Hara is on medical leave owing to long COVID. Referring to the research, she says: “You have to do it, because you are the one who is going to suffer for it if you don’t, but at the same time, you’re in bed sick.”
A plethora of symptoms
The PLRC’s survey of long COVID symptoms was the first major research study of the condition. The premise was simple enough: authors surveyed almost 3,800 people in 56 countries, many of whom were members of various long COVID support groups worldwide, including the network Body Politic, from which the PLRC originated. When the authors analysed the data, they found scores of symptoms in at least ten organ systems.
The study showed that the most prevalent problems were fatigue, post-exertional malaise — a worsening of symptoms after exertion — and the cognitive dysfunction that came to be referred to as brain fog. Nearly 86% of participants reported relapses triggered by exertion; 87% said fatigue was a main symptom; and 88% reported brain fog, with no differences in cognitive issues across age groups.
NIH launches trials for long COVID treatments: what scientists think
The paper has amassed more than 1,000 citations, been mentioned in some 60 policy statements and is widely considered a seminal paper in long COVID research, owing to its in-depth analysis. For McCorkell, however, its impact is more fundamental. “What we demonstrated with the survey is that patients can lead high-quality research, and that it’s really necessary in order to have the most comprehensive look at a condition.”
The achievement is especially notable considering that the study was conducted by unpaid volunteers, most of whom identify as disabled, and it received no financial support. By contrast, many long COVID research initiatives have tended to focus on a subset of symptoms, which comes with the risk of missing the bigger picture, says McCorkell.
“There’s a lot of complexity in these illnesses, and I think it’s really important to embrace these complexities,” says Beth Pollack, a research scientist at the Massachusetts Institute of Technology in Cambridge, whose work focuses on understanding long COVID and other infection-associated chronic illnesses. With conditions that have a range of symptoms, and for which there is only limited research, building a knowledge base starts by listening to patients’ stories and capturing the nuances of their conditions, Pollack says.
Desperate measures
In early 2020, Martha Eckey, a pharmacist in Minneapolis, Minnesota, developed a COVID-like illness. She experienced a crushing fatigue that no amount of sleep could relieve, and was bedbound for days at a time. The physicians she went to for help had no answers. In desperation, Eckey turned to the online community of people with long COVID.
She found people trying treatments from prescription medications to over-the-counter supplements. But the effectiveness of these was restricted largely to personal anecdotes.
In the hope of getting a more comprehensive, systematic understanding of what worked, Eckey designed a survey called TREAT ME, which asked people with long COVID and those with myalgic encephalomyelitis, also known as chronic fatigue syndrome (ME/CFS), about their experiences, including whether they had tried any of a list of 150 medications and supplements. More than 4,000 people responded.
Martha Eckey’s TREAT ME survey found overlap between treatments people were using for long COVID and for other chronic conditions.Credit: John Karp
Eckey found overlap with other chronic conditions. Some treatments revealed by the survey as most effective for long COVID were drugs such as beta blockers and the heart-failure medication Corlanor (ivabradine). These are sometimes used to treat postural orthostatic tachycardia syndrome, a nervous-system disorder that can be triggered by COVID-19. Eckey also found that a number of individuals reported relief after taking naltrexone, a non-opioid drug for treating substance-use disorder. When taken at low doses, it has anti-inflammatory and pain-relieving properties.
Physiotherapist David Putrino, who specializes in rehabilitation and human performance at the Icahn School of Medicine at Mount Sinai in New York City, says that the TREAT ME survey captured something both simple and profoundly important. “It’s a very fundamental question of, ‘what are you taking that’s helping right now?’” he says. The results have helped to guide his research on long COVID.
Listening to patients
TREAT ME attracted the attention of scientists and research foundations, who soon realized that this information could help to shape their efforts. One was the Open Medicine Foundation, a non-profit organization in Agoura Hills, California, that studies infection-associated chronic illnesses such as long COVID and ME/CFS.
Linda Tannenbaum, a clinical laboratory scientist, founded the Open Medicine Foundation in 2012 in response to the difficulties she encountered while seeking a diagnosis and treatment for her daughter, who has ME/CFS. Its first double-blind, randomized, placebo-controlled clinical trial will explore low-dose naltrexone (LDN) and another drug, pyridostigmine, which is used to treat an autoimmune disorder that affects voluntary muscle movements. The medications will be tested separately and in combination. Tannenbaum credits TREAT ME for helping to shape which symptoms will be assessed during the trial.
“The reason we are doing LDN as our first trial is that patients asked for it,” she says. TREAT ME also showed that many people with long COVID said that LDN helped to reduce brain fog (see go.nature.com/3qy2tpj). Given these results, the Open Medicine Foundation also incorporated parameters in the trial to test cognitive function. Both LDN and pyridostigmine have been used to treat long COVID, but as many patients report, physicians are often reluctant to prescribe these drugs because of a lack of formal, randomized, controlled trials showing their effectiveness. “Doctors are very hesitant to go outside approved, or at least medically tested, medications,” says Bateman. In her experience, insurance companies also won’t pay for these medications for people with ME/CFS and long COVID without strong evidence to support their use.
Many patient advocates say that there is insufficient clinical research on the kinds of drug that people are already using. In February, the RECOVER initiative received a further $515 million over the next 4 years to test more interventions and investigate the long-term effects of a SARS-CoV-2 infection. But so far, the only trials it has begun are of the antiviral medication Paxlovid (nirmatrelvir and ritonavir), which started enrolling patients in July 2023, and of ivabradine and intravenous immunoglobulin, which recruited its first participants last month.
Lauren Nichols, a long COVID patient advocate, helped to lead the Body Politic support group.Credit: Lauren Owens Lambert/Reuters
“There are a lot of clinical trials that are focused on more behavioural and on non-pharmaceutical interventions, and that is really not a priority to the patient community,” McCorkell says. “It is a misunderstanding of how severe the condition is, and how much of an impact on people’s quality of life it has taken.”
A spokesperson for RECOVER told Nature that the clinical trial of a computer game has already started enrolling participants and that the exercise trial is still scheduled to begin. They emphasized that these are accessible interventions, which might help some people who are affected, given the wide range of symptoms. They also said that moving these trials forwards will help in developing the framework for testing more treatments.
Lifting the fog
In the weeks after her initial COVID-19 infection, Hannah Davis found herself struggling with severe brain fog, to the point at which she could barely string two sentences together. Davis, who at the time was working as a data analyst and artist, with a particular focus on addressing biases in machine learning, kept waiting for her cognitive function to go back to normal, only for it never to return. “I had, and continue to have, terrible, terrible cognitive impairment,” says Davis, who is one of the co-founders of the PLRC.
Long COVID exercise trials proposed by NIH raise alarm
Brain fog is having a significant impact on people’s livelihoods, says Wes Ely, a physician-scientist who works in intensive care at Vanderbilt University Medical Center in Nashville, Tennessee. People with long COVID have a form of cognitive impairment that is often “like mild and moderate dementia”, he says.
Ely, who studies treatments for Alzheimer’s disease and related dementias, decided in 2020 to expand into studying the cognitive impairments associated with long COVID. He quickly recognized that the condition is deeply complex, with symptoms that go beyond cognitive impairment.
To gain a comprehensive understanding of the phenomenon, he turned to the patient community, eventually recruiting Davis and Jaime Seltzer, director of scientific and medical outreach at the non-profit organization ME Action in Santa Monica, California. Together, they drafted a clinical trial to test the medication baricitinib, an immunomodulatory drug that is used to treat rheumatoid arthritis and alopecia areata, and acute COVID-19 infections. “I wanted to learn from people who are living with this disease,” says Ely.
The trio, along with other US investigators, designed a 550-person clinical trial of baricitinib as a potential treatment for long COVID. The trial has now been funded by the NIH and will start enrolment later this year.
From Seltzer’s perspective, an effective collaboration between patients and scientists can help both sides equally, because it leads to more effective and targeted research. “We have the resources to help you do what you do even better,” Seltzer says. The lived experiences of patients can shape research priorities in several key ways, she says. These include finding the most efficient way to allocate limited funds on the basis of symptom burden; offering context on the prevalence and severity of symptoms; and identifying how the trial design can capture improvement most effectively. All of this can help lead to faster breakthroughs in treatments, which is of benefit to both patients and researchers, Seltzer says.
Microclot mystery
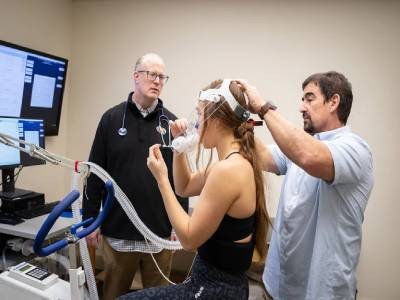
In late autumn 2022, McCorkell flew to New York City to participate in a trial being conducted by Putrino and his team. This study aimed to look for the presence of tiny blood clots, called microclots, in people with long COVID. It is thought that these cause symptoms such as fatigue and brain fog by impairing blood flow to the brain and body. There are still a lot of unknowns about microclots, including how many people with long COVID have them, how they form and whether the association is causal.
Long-COVID treatments: why the world is still waiting
McCorkell gave blood samples that were analysed using fluorescent microscopy, which confirmed she had microclots. McCorkell says it was “a wake-up call”. Until that point, she had been managing her symptoms mainly by avoiding overexertion. But the presence of the clots suggested to her that there might be active damage happening to her body. So, she started taking supplements that TREAT ME survey respondents reported as helpful.
Eckey’s results, which have not yet been published in a peer-reviewed journal, show that of 668 respondents with long COVID, between 40% and 70% found some symptom relief when taking the supplements nattokinase, serrapeptase or lumbrokinase, individually or in combination (see go.nature.com/43xgyoq).
When Putrino saw these results, he decided it was crucial to conduct clinical trials of the supplements. He expects to begin a 120-person study on lumbrokinase in the coming months, and has involved patients at every step of its development.
“Every research trial that we run, we involve the patient community in the protocol,” Putrino says. This includes taking their advice on what trials should be prioritized, what symptoms to assess, how many clinic visits to require and what the testing environment should be like, to minimize the risk of exacerbating their symptoms, he says.
McCorkell says that the supplements she’s been taking have improved her general function by about 10%. Whereas that might not sound like much, she feels it is meaningful progress. Although the long COVID research has been difficult, she sees no other option but to stay involved. “We’re driven by desperation, out of improving our own quality of life.”
Researchers at OSF HealthCare want to make sure that patients have “important conversations” about their plans for the end of their lives. Only 22% of Americans write down their end-of-life plans, according to study. A team at OSF HealthCare in Illinois is using artificial intelligence to help doctors figure out which patients are more likely to die during their hospital stay.
A news statement from OSF says that the team made an AI model that can predict a patient’s risk of dying between five and ninety days after being admitted to the hospital.
The goal is for the doctors to be able to talk to these people about important end-of-life issues.
In an interview with Fox News Digital, lead study author Dr. Jonathan Handler, an OSF HealthCare senior fellow of innovation, said, “It’s a goal of our organization that every single patient we serve would have their discussions about advanced care planning written down so that we could give them the care they want, especially at a sensitive time like the end of their life when they may not be able to talk to us because of their medical condition.”
If a patient is asleep or on a respirator, for example, it may be too late for them to tell their doctors what they want. Handler said that in an ideal world, the mortality prediction would keep patients from dying before they got the full benefits of the hospice care they could have gotten if their goals had been written down sooner.
Since the average length of a hospital stay is four days, the researchers decided to start the model at five days and end it at 90 days to give a “sense of urgency,” as one researcher put it.
The AI model was tried on a set of data from more than 75,000 people of different races, cultures, genders, and social backgrounds.
The study, which was just released in the Journal of Medical Systems, showed that the death rate for all patients was 1 in 12.
But for people who the AI model said were more likely to die while they were in the hospital, the death rate went up to one in four, which is three times higher than the average. The model was tried before and during the COVID-19 pandemic, and the results were almost the same, according to the study team.
Handler said that 13 different kinds of patient information were used to teach the patient death estimator how to work.
“That included clinical trends, like how well a patient’s organs are working, as well as how often and how intensely they’ve had to go to the health care system and other information, like their age,” he said. Handler said that the model gives a doctor a chance, or “confidence level,” as well as an account of why the patient has a higher-than-normal chance of dying.
“At the end of the day, the AI takes a lot of information that would take a clinician a long time to gather, analyze, and summarize on their own, and then presents that information along with the prediction to allow the clinician to make a decision,” he said. Handler said that a similar AI model made at NYU Langone gave the OSF researchers an idea of what they could do.
“They had made a death predictor for the first 60 days, which we tried to copy,” he said.
“We think our population is very different from theirs, so we used a different kind of predictor to get the results we wanted, and we were successful.”
“Then, the AI uses this information to figure out how likely it is that the patient will die in the next five to ninety days.”
The forecast “isn’t perfect,” Handler said. Just because it shows a higher risk of death doesn’t mean it will happen.
“But at the end of the day, the goal is to get the clinician to talk, even if the predictor is wrong,” he said. “In the end, we want to do what the patient wants and give them the care they need at the end of life,” Handler said. OSF is already using the AI tool because, as Handler said, the health care system “tried to integrate it as smoothly as possible into the clinicians’ workflow in a way that helps them.”
Handler said, “We are now in the process of optimizing the tool to make sure it has the most impact and helps patients and clinicians have a deep, meaningful, and thoughtful conversation.”
Expert on AI points out possible limits
Dr. Harvey Castro, a board-certified emergency medicine doctor in Dallas, Texas, and a national speaker on AI in health care, said that OSF’s model may have some benefits, but it may also have some risks and limits.
Possible fake results is one of them. “If the AI model wrongly predicts that a patient is at a high risk of dying when they are not, it could cause the patient and their family needless stress,” Castro said. Castro also brought up the risk of false positives.
“If the AI model doesn’t find a patient who is at high risk of dying, important conversations about end-of-life care might be put off or never happen,” he said. “If this happens, the patient might not get the care they would have wanted in their last days.”
Castro said that other possible risks include relying too much on AI, worrying about data privacy, and the possibility of bias if the model is built on a small set of data. This could lead to different care advice for different patient groups.
The expert said that these kinds of models should be used with human contact.
“End-of-life conversations are difficult and can have big effects on a patient’s mind,” he said. “People who work in health care should use AI predictions along with a human touch.”
The expert said that these models need to be constantly checked and given feedback to make sure they are still accurate and useful in the real world.
“It is very important to study AI’s role in health care from an ethical point of view, especially when making predictions about life and death.”










{kind=link}
{kind=link}